Introduction
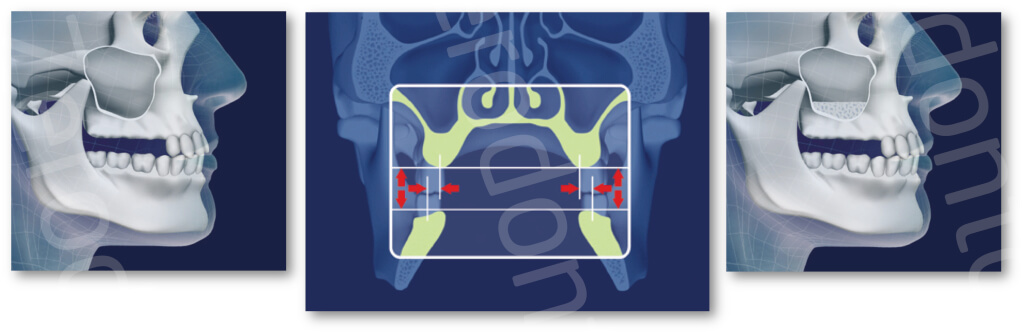
The physiological resorption of alveolar process in the corono-apical and vestibular-palatal direction following tooth loss often does not allow the positioning of implants in the posterior part of the upper jaw without an adequate bone reconstruction. The functional load exerted on the residual crest which transforms into compression force favors centripetal and cranio-caudal bone resorption (Cawood et al. 1988) with consequent reduction in size of the alveolar process associated with a progressive pneumatization of the maxillary sinus.
Among the pre-implant surgical procedures for bone reconstruction, the maxillary sinus surgery has been shown to have a high clinical predictability (Wallace et al. 2003,Del Fabbro et al. 2004-2008-2012-2013 a-b, Pjetursson et al. 2008, Testori et al. 2012). Historically in cases of bone atrophy where the residual bone is less than 4 mm, the lateral approach was utilized.

in cases of minor atrophy where the bone crest height is over 4 mm, a less invasive technique can be used involving a crestal approach first described by Summers (Summers 1994) later revised by numerous authors (Del Fabbro et al. 2012). However, this clinical view is under scrutiny by many clinicians since the diagnostic algorithm involved many variables.
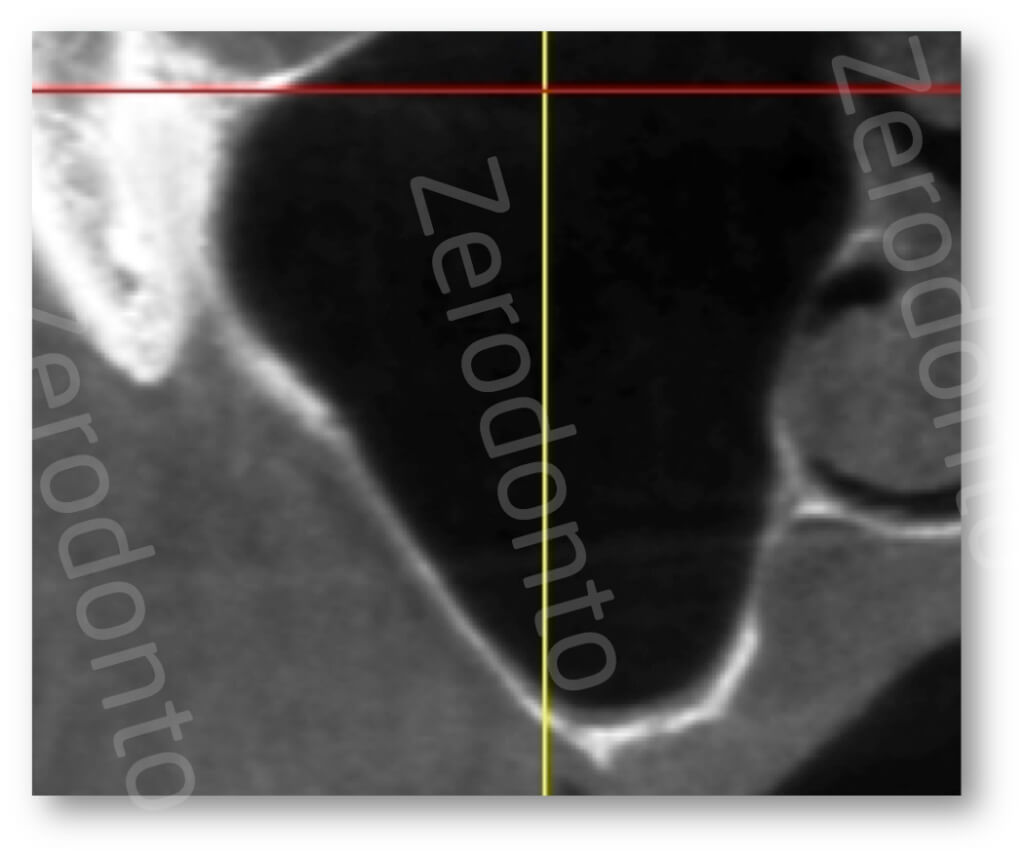
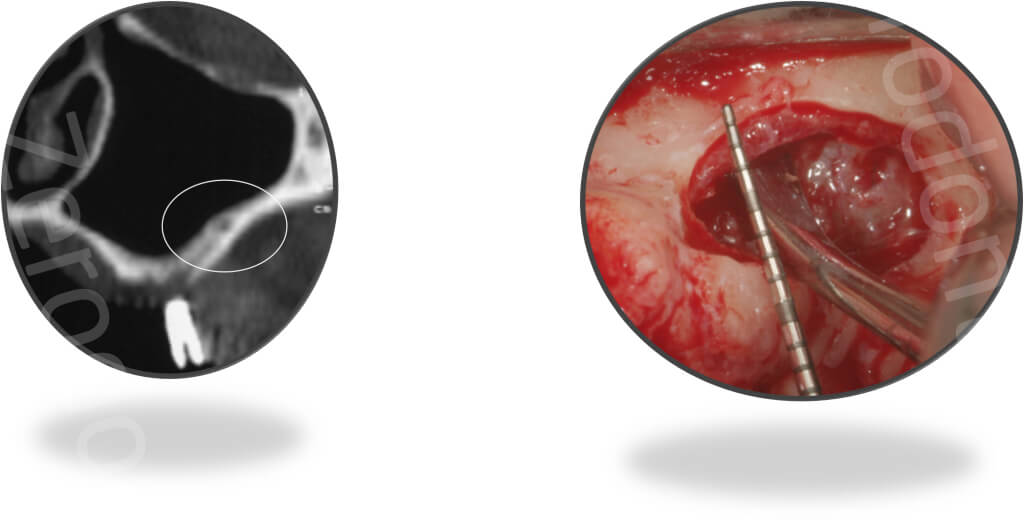
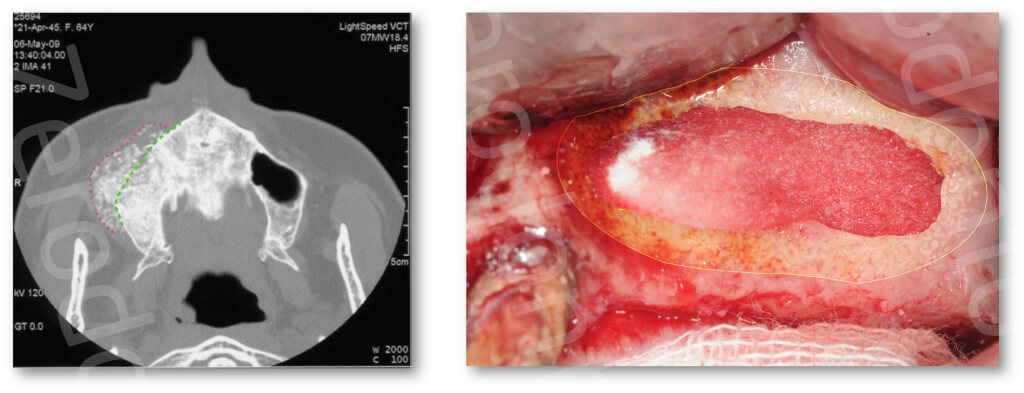
In the planning stage it is important to consider, besides having a good knowledge of the anatomy and physiology of maxillary sinus, naso-sinusal diseases, which must be diagnosed before the operation and in some cases assessed together with an ENT specialist. During this precautionary diagnosis phase, all the conditions, from the point of view of ENT specialist, that may be contraindicated for sinus elevation (Mantovani M et al. 2005), can be identified via specific, 3-D radiological examination such as a CT or CBCT which is currently the most suitable exam due to the low doses of radiation absorbed by the patient (Ludlow et al. 2008).
Surgical Protocols – Lateral Approach
1) Appropriate anesthesia
A proper anesthesia technique is a fundamental prerequisite for an effective surgical procedure requiring a slow, deep injection (1 ml/min) that does not expand the tissues and change the morphology of the fornix, to obtain a long-lasting, effective anesthesia. The drug of choice is Articaine Hydrochloride 4% with Adrenaline 1: 100,000 which has an onset of about 2 minutes (Costa et al. 2005). Anesthesia starts with injection beginning from the disto-vestibular level and continuingwith mesio-vestibular and disto-palatal levels, the corner of the mouth is anesthetized as well to allow the surgeon to efficiently retract the checks without causing discomfort to the patient.
2) Flap design
Before creating the access flap, the following points must be taken into consideration:
- mesio-distal position of sinus
- ideal position of antrostomy
- position and quantity of keratinized tissue
- presence/absence of teeth
The flap must be wider than the extension of the sinus on the buccal wall.
The incision is full-thickness and may be crestal or more towards the palate, the latter variant is recommended if there is a muscular insertion on the ridge or if the keratined tissue is insufficient (less than 2 to 3 mm) from the center of the ridge to the mucogingival joint. The presence of keratinized tissue on both edges of the incision aids suturing. The palatal extension must maintain vascular support and avoid necrosis in the palatal portion of the flap. If the sinus extends into the canine area, a hockey-stick incision should be made that is mesial to the canine, full thickness into keratined tissue starting from the line-angle of the tooth,

and partial thickness in alveolar mucosa to avoid neurological injuries to the infraorbital nerve.

If the sinus is located in the first/second premolar area, the incision will begin distal to the canine. Depending on the clinical situation, the incision may be intrasulcular or paramarginal, the former is recommended if there are natural teeth with no periodontal disease and ends with a microsurgical suturing technique. If conventional fixed prostheses on natural teeth are present a paramarginal incision apical to the probing depth is preferred, especially in the event of thin periodontal biotypes. If bone is to be taken from the tuber, the crestal incision can reach it to allow the simultaneous exposure of the donor site. The vertical releasing incision must be made parallel to vascularization and depends on the extension of the sinus on the vestibular bone wall and the position of the planned antrostomy.
3) Flap elevation
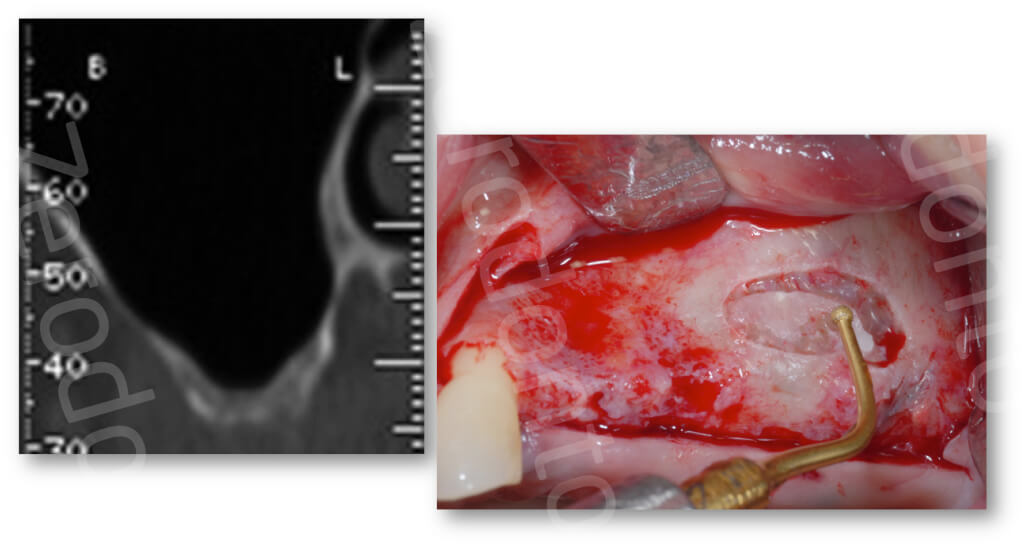
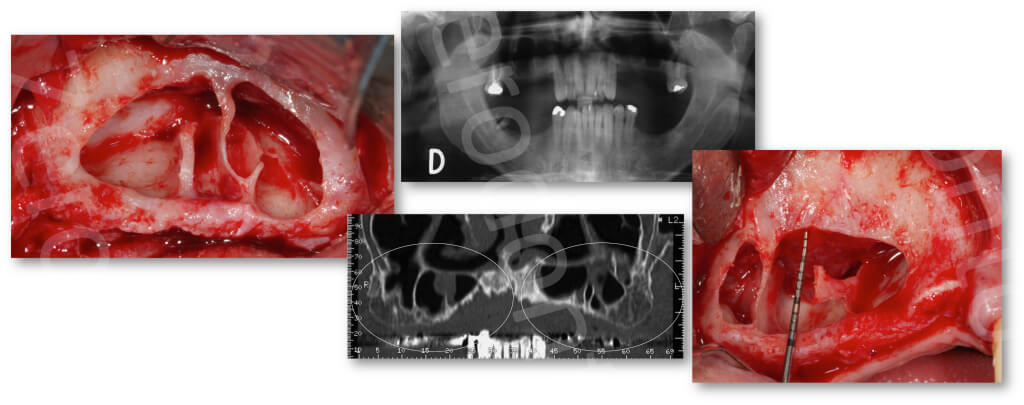
The full thickness flap must be elevated with on a flap elevator that must be adherent to the bone so that the periosteum remains undamaged. Correct flap design and elevation allow excellent control of hemostasis, which in turn depends on several factors like general medical condition of the patients, and anesthesia technique used. Once the bone plane can be seen, a compact bone part (which is not bleeding) can be identified; the underlying marrow areas will bleed lightly. In some cases, the posterior-superior alveolar artery anastomosis with the infraorbital artery can be seen. If the area bleeds excessively, a gauze compress can be appliedfor 5 minutes on the vestibular fornix. In cases where the presurgery computerized tomograph(CT) shows a lack of vestibular compact bone, the surgeon must proceed with caution during detachment, carefully dissecting the mucosal flap of the sinus membrane.
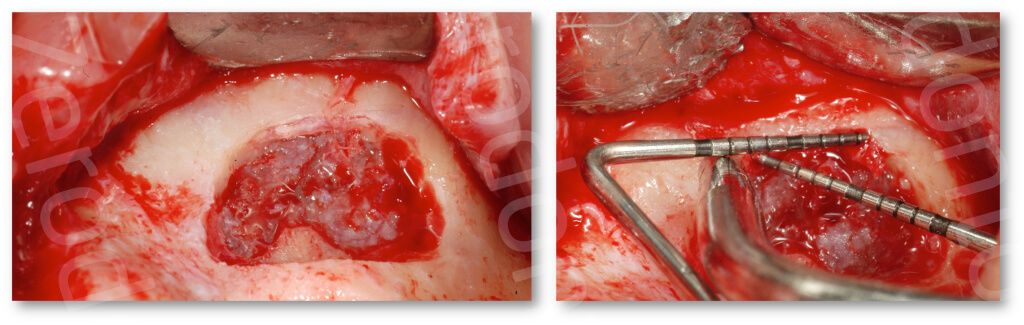
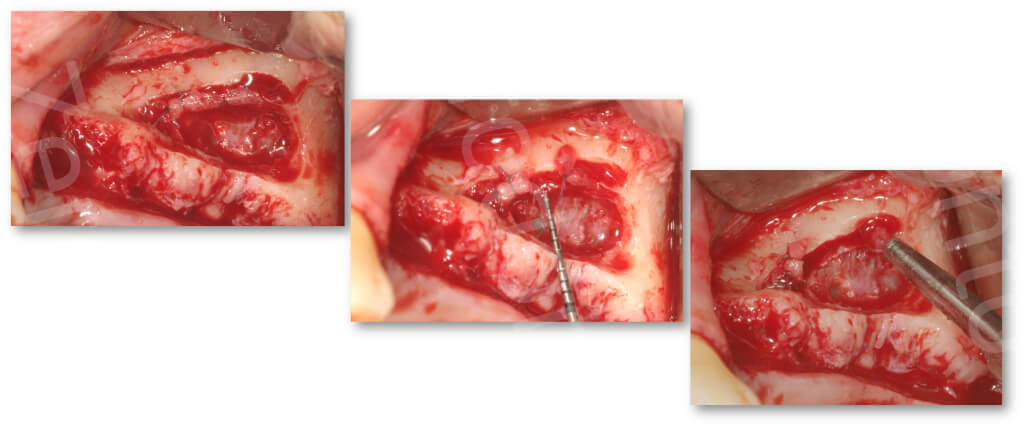
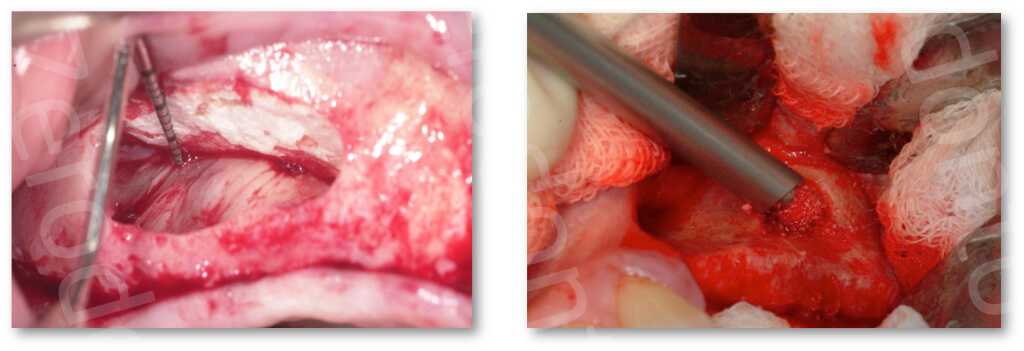
4) Antrostomy
The position of the antrostomy is determinedby the extension of the maxillary sinus. The antrostomy can easily be carried out with abundant irrigation by cooled, physiological solution, using a high-speed (40,000 rpm) straight handpiece and a tungsten carbide bur, diameter ISO 1.8, close to the sinus membranewhen the color of the membrane begins to turn blue, amedium grit diamond burISO 1.8 is recommended which is less traumatic in the event of accidental contact with the thin sinus membrane.If the compact bone is thin and the membrane turns blue as soon as the flap has been detached, the authors suggest using a medium grit diamond bur immediately.
It is possible to use a piezoelectric technique to carry out the antrostomy, which reduces the possibility of accidental perforations (Vercellotti et al. 2001).
If the bone wall is more than 1 mm thick, the bone can be reduced using an osteoplastic piezoelectric insert
to collect bone that will be used as graft material.
Antrostomy is normally oval in shape without sharp edges that could lead to perforationof the Schneiderian membrane during the later operation stages. The shape may vary depending on the presence of septa, even becoming kidney-shaped in order to manage the presence of anymaxillary septa (also calledUnderwood’s septa) efficiently. Also, the antrostomy can be divided into two separate osteotomies or, in some cases, it is possible to cut off the base of the septum and lift it completely.
The size of the antrostomy depends on the number of implants that must be inserted and on the vertical elevation to be achieved. On average, a size of 20 mm mesio-distally and 15 mm apico-coronallyis enough to guarantee easy surgical access. It is advisable to reduce the size of the antrostomy when the operator’s learning curve has reached a level that allows carrying out a correct surgical procedure even with a smaller antrostomy. A more conservative access allows bone tissue to be saved, which will aid graft healing centripetally from the walls to the center of the graft.
The technique can be modified in relation to the position and the course of the vascular anastomosis; if the surgeon knows where the artery is, the antrostomy should be made more coronally.
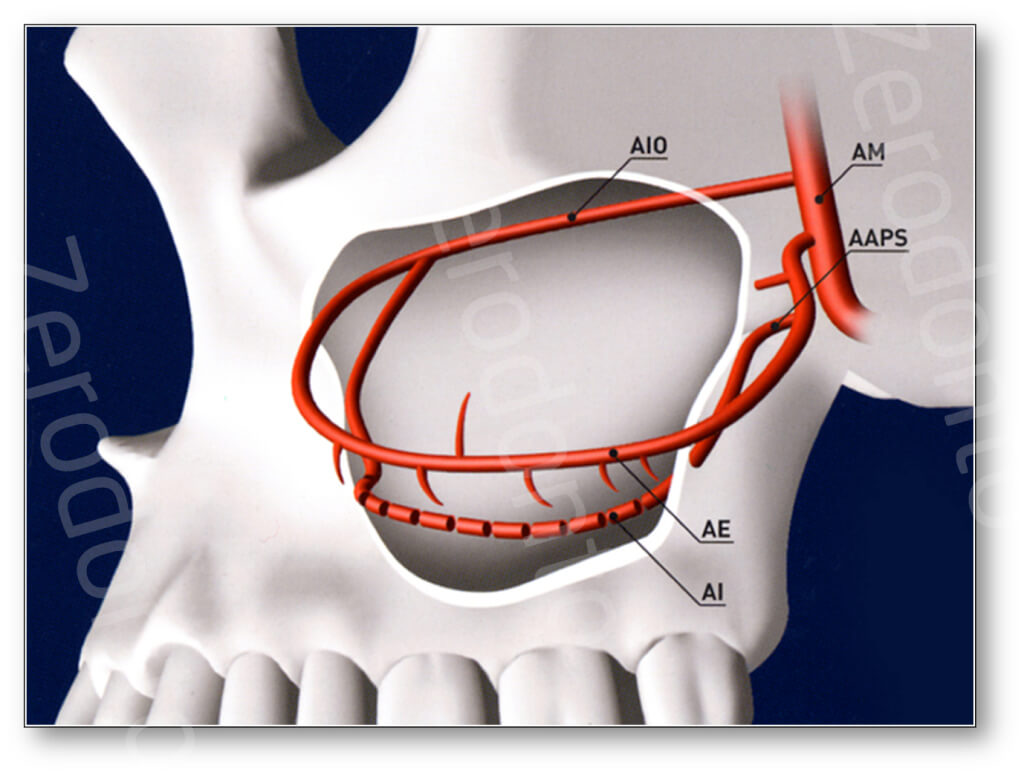
If the artery is in the way of the planned antrostomy, we suggest severing the vessel (Testori et al 2013).
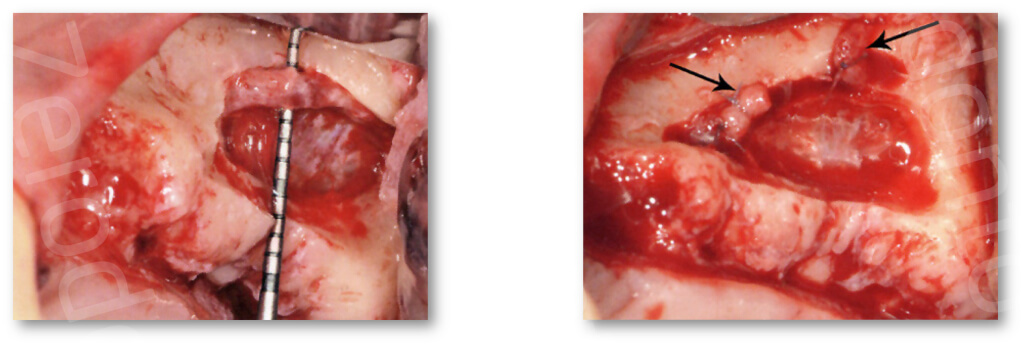
If the vessel pathway is extraosseous, which can be clinically verified, the vessel will stay adhered to the sinus membrane and will be lifted together with it.
To avoid bleeding during and after surgery, it is necessary to electro- cauterize the two trunks of the vessels severed during the operation with specific bipolar devices or to use bone wax (Bone Wax, Johnson &Johnson, Bruxelles, Belgium) on each end or ligate it in case of wider vessel (> 2 mm) (Testori et al 2013).
Once the vasoconstrictive effect of the local anesthesia has ended, a severed but untreated anastomosis may cause hemorrhaging after suturing or after the patient has been discharged.
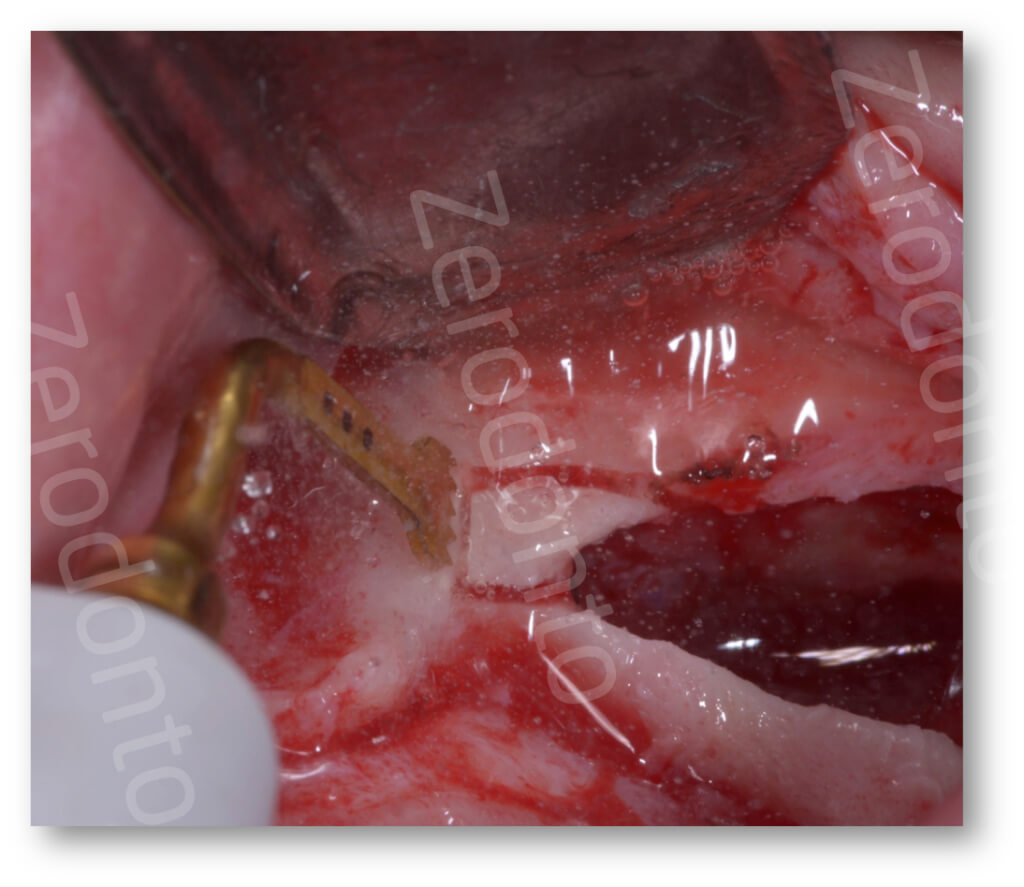
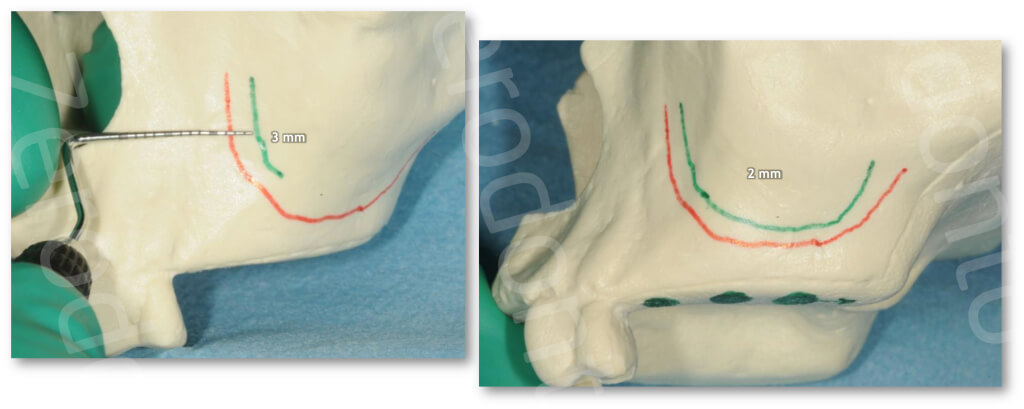
The distal margin of the antrostomyis positioned in relation to the number of implants to be inserted. The coronal marginof the antrostomy must be 3 mm apical to the floor of the sinus.The mesial edge of the antrostomy must be as far forward as possible as the anterior recess is usually narrower and may lead to on higher rate of perforation.
Once the osteotomy has been completed, the mobility of the bone segment is tested by pressing slightly on the edges. Any residual bone bridges must be removed along the antrostomy perimeter as their sharp edges may cause membrane perforation if they are violated towards the interior.
The antrostomy may be divided into antrostomy by reflection in cases where the vestibular bone wall is < 1 mm thick and it is left adherent to the Schneiderianmembrane, and turned inside the maxillary sinus, acting as the future antrum floor. If the bone is thicker than 1 mm, it is easier to erode the vestibular wall (antrostomy by erosion) (Smiler 1997).Trying to elevate a healthy sinus membrane 100/500 microns thick attached to a bony wall thicker than 1 mm could easily result in a perforation.
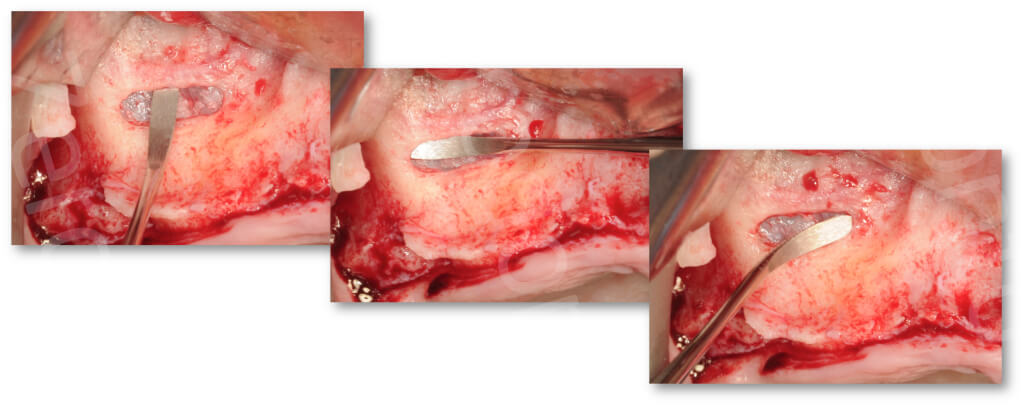
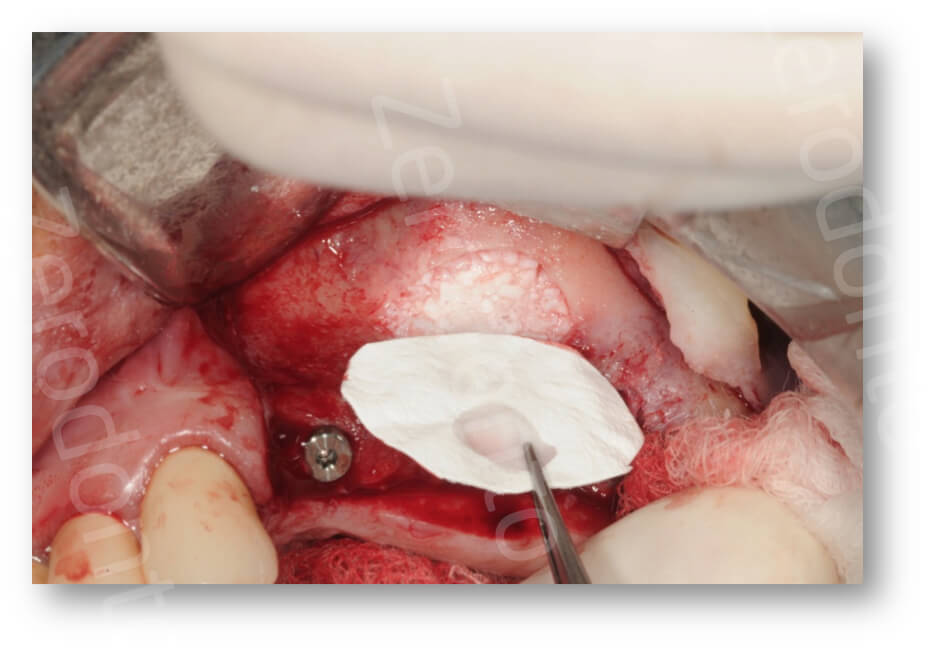
5) Elevation of sinus membrane
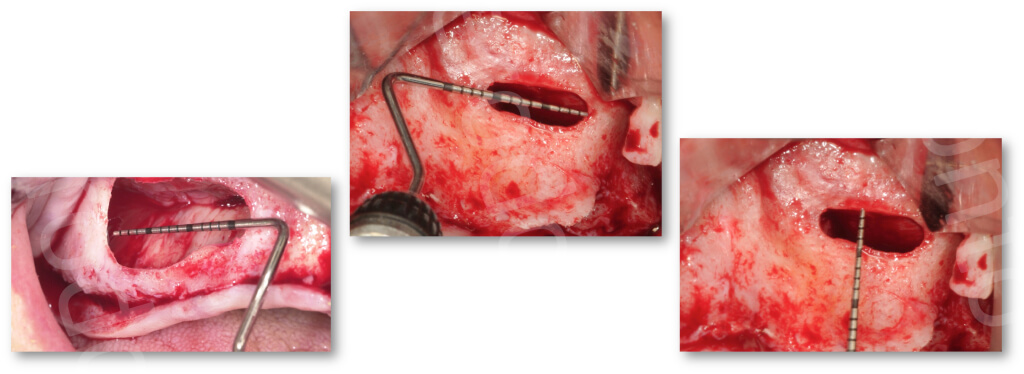
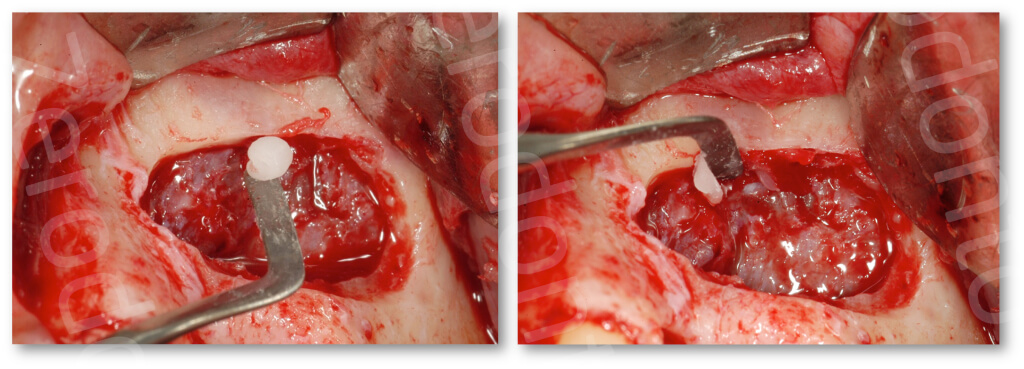
Once the antrostomy has been completed, a dedicated piezoelectric insert is used to locate a cleavage plane between the bone and periostal side of the sinus membrane along the margins of the antrostomy.
The elevation is the carried out using manual surgical tools which are easier to handle compared to the piezoelectric insert. Tools must stay in contact with the bone applying constant, continuous pressure to elevate the membrane without perforating it.
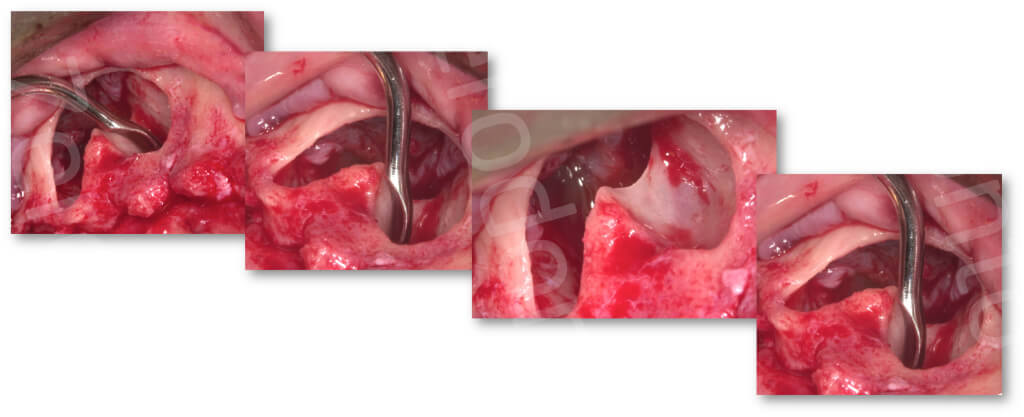
The detachment of the sinus membrane must proceed where there is less resistance starting from the upper margin of the antrostomy and continuing distally, mesially and finally coronally. In case of resistance, it is advisable to keep to the underlying bone layer and sever the adherence utilizing a sharp instrument.
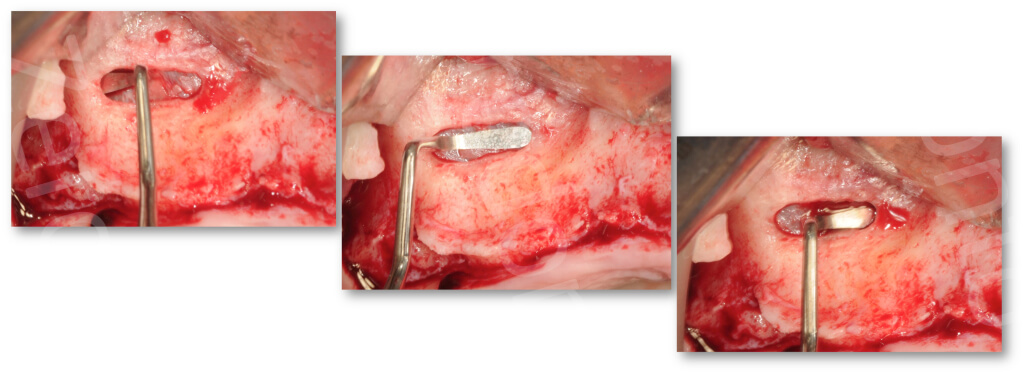
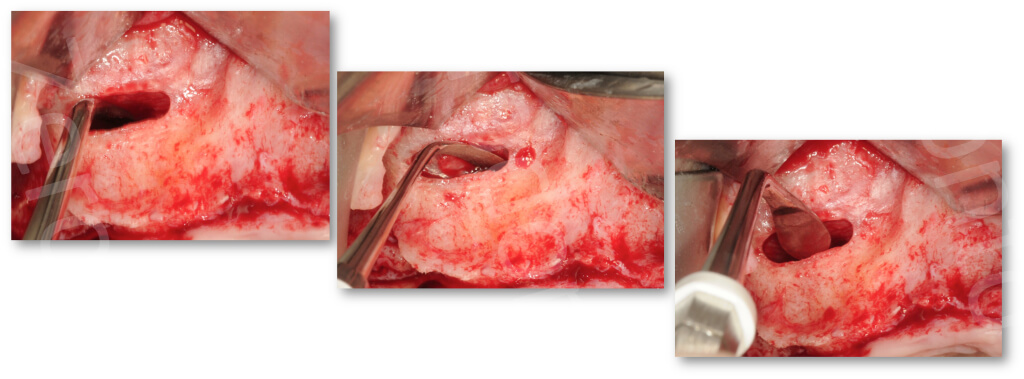
The mucosa must be detached until the medial wall (lateral wall of the nose) of the sinus cavity is exposed. Lateralization of the maxillary sinus without detachment of the medial wall as a consequence of repneumatization of the sinus may lead to mobilization of the graft material. Detachment until the medial wall permits exposing a larger bone surface, which favors better recovery of the graft (Margolin et al. 1998), and implant positioning that is more favorable for prosthetic rehabilitation.

Elevation must be carried out with dedicated tools and not with graft material that must be passively positioned in the recreated volume without further membrane detachment. The creation of a predetermined volume is a fundamental prerequisite of the surgical technique to prevent accidental perforations by materials that may remain undetected and cause dispersion of the graft material in the sinus cavity.
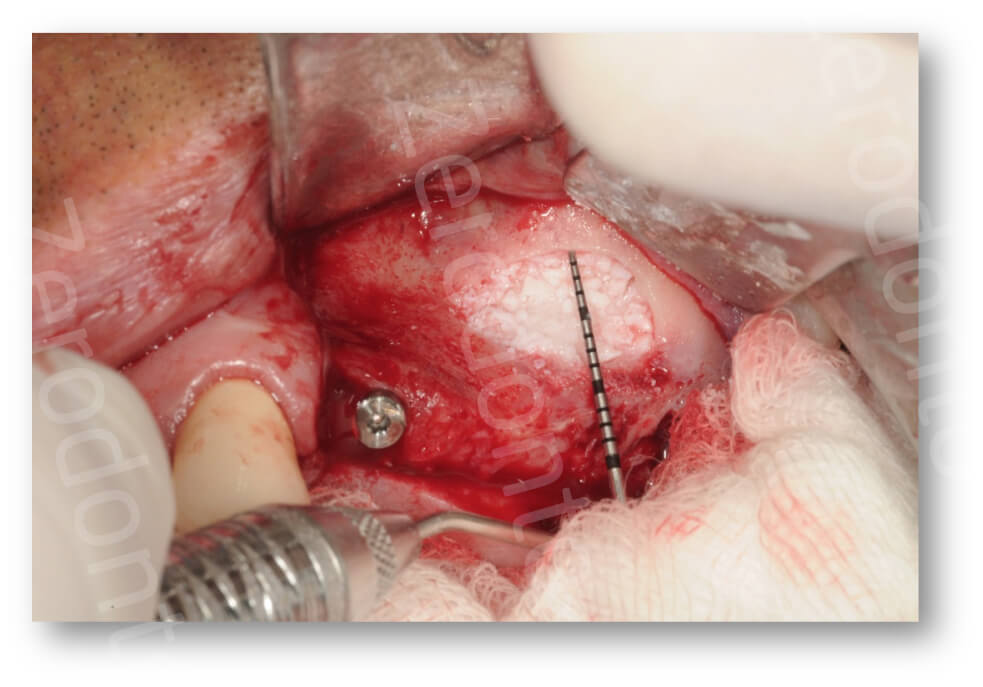
6) Preparation of implant site
After lifting the sinus membrane, it is possible to position the implants at the same time if the bone height is about 3-4 mm. In clinical cases with type 3 and 4 bones on the bone ridge, we recommend undersizing the implant site. While preparing the implant sites with the burs, the surgeon must protect the sinus membrane with a periosteum-elevator or a collagen sponge inside the subsinus cavity to avoid damaging it with the burs. If bone thickness is less than 3 or 4 mm, it is advisable to elevate the sinus and place the implants once the graft has consolidated. A systematic review (Del Fabbro et al. 2004) showed that there are no statistically significant differences in implants positioned at the same time as elevation and after graft consolidation.
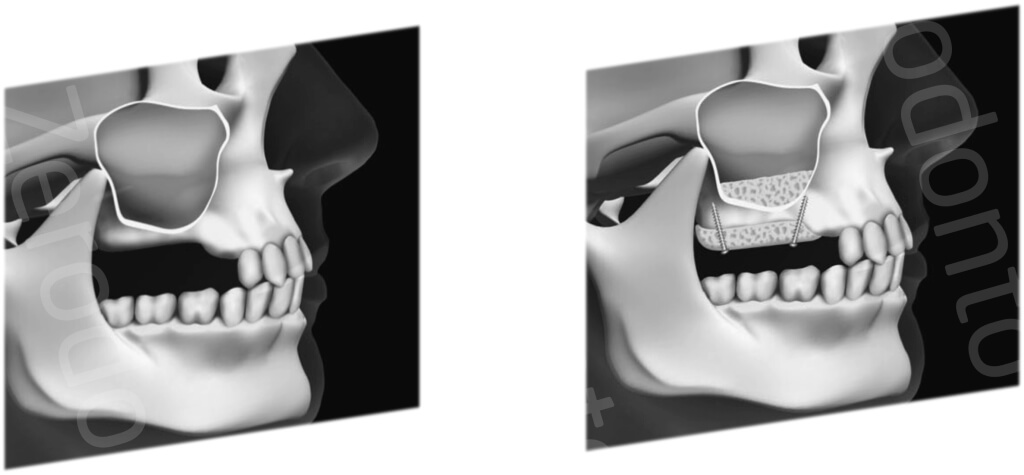
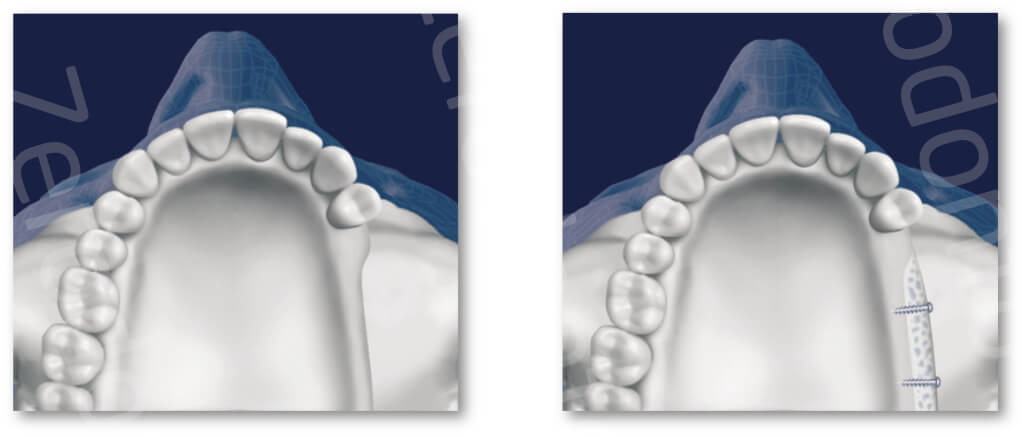
7) Insertion of graft material and implant positioning in the case of simultaneous approach
Also in the absence of perforations, it is advisable to insert a non cross-linked, resorbable membrane to avoid, during the compacting of the graft, that some biomaterial particles, especially if using granules of 1-2 mm diameter, causing micro perforations. Currently we do not know if these micro perforations are clinically relevant, nevertheless it is reasonable to recommend preserving sinus membrane’s anatomy and function. A recent histological study on humans showed that the percentage of vital bone is higher when large-granule (1-2 mm) deproteinized, bovine bone is used compared to small-granule (0.5 – 1 mm) (Testori et al. 2013). The graft must be inserted starting from the less accessible areas, hence, in the anterior and posterior recesses, and then along the medial wall of the sinus, positioning the graft in contact with bone to facilitate recovery.
If simultaneous implant positioning is planned, 2/3 of the graft is placed and then the implants are placed and finally the central space is filled in.
In patients with thin parodontal biotype, or those wearing removable prosthesis, it is advisable to place the implants subcrestally.
Excessive compacting of the graft material reduces the space between biomaterial particles and impairs vascularization; this is particularly marked with slow reabsorbing biomaterials. Placement of implants with rough surface significantly increases the percentage of bone-implant contact and also the survival rate is higher with respect to smooth surfaces.
Once the sinus cavity has been filled, a resorbable membrane is positioned on the vestibular bone wall at the antrostomy level. Some clinical studies (Tarnow et al. 2000; Tawill et al. 2001) suggested that positioning a resorbable membrane on the antrostomy determines a higher percentage of vital bone and implant successcompared to sites that did not have a membrane placed. A recent paper (Barone et al. 2013) reported data that contrasted previous findings arguing that there is no statistically significant difference in the percentage of vital bone whether a membrane was used or not. A recent metanalisys showed that a membrane over the window does not increase the prognosis of the procedure (Torres Garcia-Denche et al. 2013). A new approach involves the positioning of a membrane sagging 2mm into the antrostomy to prevent graft material from seeping out in case of accidental increase in intra-sinus pressure (Testori et al. 2013). Autogenous bone has always been considered the gold standardas graft material for its osteogenic, osteoinductive and osteoconductive capacity and it’s for this reason that it is recommended during the development of the technique. So far no statistically significant differences have been reported between the use autogenous bone and bone substitute as regards implant survival (Wallace et al. 2012). However there is no doubt that rough implant surface plays an important role on the final clinical outcome. The most promising family of biomaterials are the xenografts whose success can be attributed to three factors:
- Osteoconductivity of the biomaterial which determines about 25% of the vital bone 6-8 months after grafting.
- The slow resorption adds 25% more mineral content to the future implant site.
- Histological studies show that residual biomaterial particles never make direct contact with the implant surface but are surrounded and interconnected by the process of bone bridging (Wallace et al. 2012).
Clinical data, histological studies and reduced invasivity of the surgical procedure, in the absence of a donor site, seem to suggest that currently biomaterials are the gold standard in this type of surgery. There is histological evidence and clinical studies that show how the maturation of the graft can be accelerated by mixing autogenous bone with synthetic biomaterials even if invasivity tends to go up (Wallace et al. 2012).
It is worth noting that high success rates have been reported using alloplastic materials even though solid scientific evidence has been reported (Wallace et al. 2012) less frequently
Over the last decade we have seen the introduction of biotechnologies using morphogenetic proteins and recombinant growth factors. To this day these have not been approved for clinical use in Europe besides the fact that they possess certain negative aspects: high cost, presence of immature bone in the earlier stages of graft recovery and resorption of the graft itself. To reduce the resorption of the graft a certain amount of homologous bone is added (Tarnow et al. 2010) obtaining promising results, or xenografts with a high stability of size even if, in some cases, they had worse histological results compared to using xenografts alone (Kao et al. 2012). Using recombinant growth factors in association with deproteinized bovine bone produced good results in soft tissue healing and improvement in the healing of the graft itself (Froum et al. 2013). In the case of homologous growth factors, some studies have highlighted a positive effect also in hard tissues; on the other hand, recent systematic reviews associated the positive effect to soft tissues in particular. A recent systematic analysis on the effectiveness of growth factors in maxillary sinus elevation considered 12 papers comprising a total of 445 maxillary sinus elevations (Del Fabbro et al. 2013). Six of these studies, based on histomorphometric analysis reported a positive effect platelet concentration on bone regeneration. On the contrary, other six studies showed no significant difference between the control group and test group using growth factors. Unfortunately these studies are hard to compare as they varied widely regarding study design, surgical procedures, type of graft utilized, and other variables they considered in their clinical and histomorphometric analyses. All the studies agreed on the positive effect of the growth factors in the healing of soft tissues and less post-op discomfort. These data have been reported but not quantified hence preventing a meta-analysis.
In conclusion currently there is no evident advantage to using growth factors in maxillary sinus elevation and further, randomized, standardized studies are necessary. An alternative technique has been reported (Lundgren et al. 2004, Cricchio et al. 2011) which, in simultaneous implant placement, suggests using only blood clot or collagen or only homologous growth factors (Mazor et al. 2009) placed under the sinus membrane. The rationale behind this approach is that the implants create a curtain effect supporting the membrane and favoring new inter-implant bone formation.
In cases where no filler material is used, bone regeneration is localized up to the implant apex or slightly more coronal, at times leaving the last screws, which radiologically seem to protrude into the sinus, in contact with the sinus membrane.
The clinical approach used by the authors is based on systematic reviews found in literature where it is shown that favorable prognostic factors for clinical success are:
- rough implant surface
- biomaterials, especially xenografts
- positioning of a membrane on the antrostomy
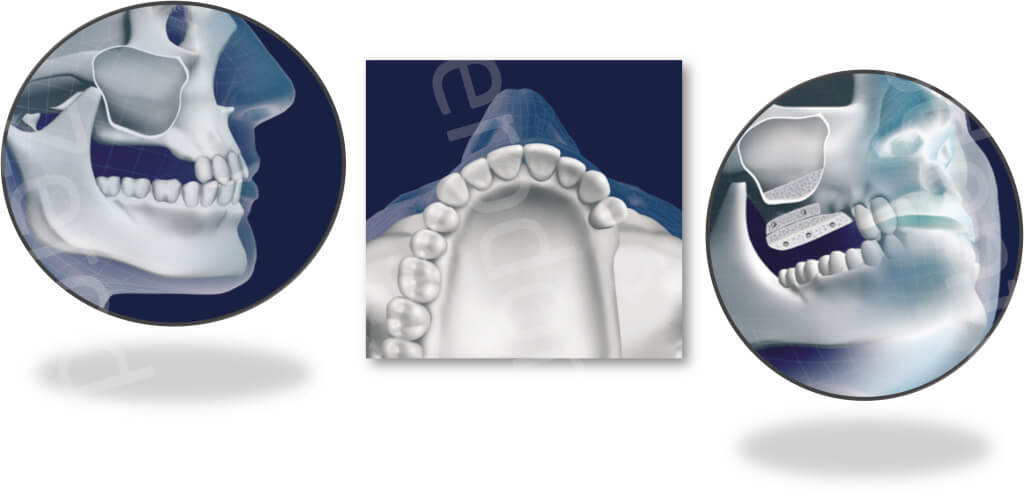
Finally in cases of maxillary sinus elevation using only biomaterials, we suggest waiting 6 to 9 months before positioning the implants when the deferred approach is adopted or before carrying out the second stage when the simultaneous approach is chosen.
8) Suture
The flap must be sutured without tension; if necessary, periosteal releasing incisions can be made to achieve flap passivity. The first suture must be carried out at the apical portion of the vertical releasing incision.
Horizontal mattress stitches or continuous sutures can be used at the crest.
The type of suture to be used depends on the type of tissue: non-resorbable monofilament is recommended in keratinized tissue, while resorbable sutures are recommended for the alveolar mucosa, as an alternative only resorbable sutures can be used.
9) What are the most appropriate clinical recommendations to reduce the incidence of post-op complications?
- (i)careful assessment of the medical history of the patient
- (ii) proper patient selection with healthy maxillary sinus
- (iii) a pre-operative CT scan to evaluate sinus anatomy and identify preexisting pathology
- (iv) recommendation of a smoking cessation protocol and, especially in case of heavy smokers (≥15 cigarettes a day), careful assessment carried out
- (v) preventive resolution of periodontal and endodontic diseases
- (vi) adequate antibiotic prophylaxis
- (vii) achievement of full mouth plaque score (FMPS) and full mouth bleeding score (FMB5) <15%. In case of provisional crowns it is advisable to remove the temporary crowns and disinfect the abutments with antiseptic solution
- (viii) pre-op disinfection of the skin with an antiseptic solution and mouth rinses with chlorhexidine
- (ix) use of sterile draping and infection-control protocol
- (x) keeping the incision distant from the antrostomy
- (xi) salivary-contamination prevention for bone graft and/or other biomaterials
- (xii) intra- and postoperative control of the hemostasis
- (xiii) prevention of bone overheating
- (xiv) use of two different surgical sets of instruments: one for the flap elevation phase and the other for the grafting phase
- (xv) rinsing the surgical field with sterile saline solution
- (xvi) keeping the surgical time as short as possible
- (xvii) postoperative chlorhexidine rinses
- (xviii) appropriate postoperative pharmacological therapy
- (xix) preplanned check-ups: weekly for the first month and monthly for the following 3 months
REFERENCES
- Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral Maxillofac Surg. 1988;17:233-236.
- Wallace SS, Froum SJ. Effect of maxillary augmentation of survival of endosseous dental implants. A systematic review. Ann Periodontol. 2003;8 328-343.
- Del Fabbro M, Testori T, Francetti L, Weinstein RL. Systematic review of survival rates for implants placed in the grafted maxillary sinus. J Periodontics Restorative Dent. 2004;24:565-577.
- Del Fabbro M, Rosano G, Taschieri S. Implant survival rates after maxillary sinus augmentation. Eur J Oral Sci 2008;116:497-506.
- Del Fabbro M, Corbella S, Weinstein T, Ceresoli V, Taschieri S. Implant survival rates after osteotome-mediated maxillary sinus augmentation: a systematic review. Clin Implant Dent Relat Res. 2012;14:s159-168.
- Del Fabbro M, Bortolin M, Taschieri S, Weinstein RL. Effect of autologous growth factors in maxillary sinus augmentation: a systematic review. Clin Implant Dent Relat Res. 2013a;15:205-216.
- Del Fabbro M, Wallace SS, Testori T. Long-term implant survival in the grafted maxillary sinus: a systematic review. Int J Periodontics Rest Dent 2013b;33:773-783.
- Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. Part I: lateral approach J Periodontol. 2008;35:216-240.
- Testori T, Weinstein RL, Taschieri S, Del Fabbro M. Risk factor analysis following maxillary sinus augmentation: a retrospective multicenter study. Int J Oral Maxillofac Implants. 2012;27:1170-1176.
- Testori T, Drago L, Wallace SS, Capelli M, Galli F, Zuffetti F, Parenti A, Deflorian M, Fumagalli L, Weinstein RL, Maiorana C, Di Stefano D, Valentini P, Giannì AB, Chiapasco M, Vinci R, Pignataro L, Mantovani M, Torretta S, Pipolo C, Felisati G, Padoan G, Castelnuovo P, Mattina R, Del Fabbro M. Prevention and treatment of postoperative infections after sinus elevation surgery: clinical consensus and recommendations. Int J Dent. 2012;2012:365809. doi: 10.1155/2012/365809. Epub 2012 Aug 9.
- Summers RB. A new concept in maxillary implant surgery: the osteotome technique. Compendium of Continuing Education in Dentistry. 1994a;15-152-160.
- Del Fabbro M, Corbella S, Weinstein T, Ceresoli V, Taschieri S. Implant survival rates after osteotome-mediated maxillary sinus augmentation: a systematic review. Clin Implant Dent Relat Res. 2012;14:s159-168.
- Mantovani M. Implicazioni otorinolaringoiatriche nell’elevazione del seno mascellare. In: La chirurgia del seno mascellare e le alternative terapeutiche. Testori T, Weinstein R, Wallace SS. Viterbo Acme, 2005
- Ludlow J, Ivanovic M. Comparative dosimetry of dental CBCT devices and 64-slice CT for oral and maxillofacial radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:106-114.
- Costa CG, Tortamano IP, Rocha RG, Francischone CE, Tortamano N. Onset and duration periods of articaine and lidocaine on maxillary infiltration. Quintessence Int. 2005;36:197-201.
- Vercellotti T, De Paoli S, Nevins M. The piezoelectric bony window osteotomy and sinus membrane elevation: introduction of a new technique for simplification of the sinus augmentation procedure. Int J Periodontics Restorative Dent. 2001; 21: 561-7.
- Testori T, Rosano G, Taschieri S, Del Fabbro M. Ligation of an unusually large vessel during maxillary sinus floor augmentation. A case report. Eur J Oral Implantol 2010;3:255-8.
- Smiler D.G. The sinus lift graft: basic technique and variations Periodontics Aesthet. Dent. 1997; 9: 885-93.
- Margolin MD, Cogan AG, Taylor M, Buck D, McAllister TN, Toth C, McAllister BS. Maxillary sinus augmentation in the non-human primate: a comparative radiographic and histologic study between recombinant human osteogenic protein-1 and natural bone mineral. J Periodontol. 1998;69:911-919.
- Del Fabbro M, Testori T, Francetti L, Weinstein RL. Systematic review of survival rates for implants placed in the grafted maxillary sinus. J Periodontics Restorative Dent. 2004;24:565-577.
- Testori T, Rosano G, Taschieri S, Del Fabbro M. Ligation of an unusually large vessel during maxillary sinus floor augmentation. A case report. Eur J Oral Implantol 2010;3:255-8.
- Tarnow DP, Wallace SS, Froum SJ, Roher MD, Cho S-C. Histologic and clinical comparison of bilateral sinus floor elevations with and without barrier membrane placement in 12 patients: Part 3 of an ongoing prospective study. Int J Periodontics Restorative Dent. 2000;20:117-121.
- Tawill G, Mawla M. Sinus floor elevation using a bovine bone mineral (bio-oss) with or without the concomitant use of bilayered collagen barrier (Bio-Gide): a clinical report of immediate and delayed implant placement. Int J Oral Maxillofac Implants. 2001;16:713-721.
- Barone A, Ricci M, Grassi RF, Nannmark U, Quaranta A, Covani U. A 6-month histological analysis on maxillary sinus augmentation with and without use of collagen membranes over the osteotomy window: randomized clinical trial. Clin Oral Implants Res. 2013;24:1-6.
- García-Denche JT, Wu X, Martinez PP, Eimar H, Ikbal DJ, Hernández G, López-Cabarcos E, Fernandez-Tresguerres I, Tamimi F. Membranes over the lateral window in sinus augmentation procedures: a two-arm and split-mouth randomized clinical trials. J Clin Periodontol. 2013 Nov;40:1043-51.
- Testori T, Mandelli F, Weinstein RL, Valentini P, Wallace SS. A novel technique to prevent the loss of graft material through the antrostomy after sinus surgery: a technical note. Int J Oral Maxillofac Implants. submitted 2013.
- Wallace SS, Tarnow DP, Froum SJ, Cho SC, Zadeh HH, Stoupel J, Del Fabbro M, Testori T. Maxillary sinus elevation by lateral window approach: evolution of technology and technique. J Evid Based Dent Pract. 2012;12:161-71.
- Tarnow DP, Wallace SS, Testori T, Froum SJ, Motroni A, Prasad HS. Maxillary sinus augmentation using recombinant bone morphogenetic protein-2/acellular collagen sponge in combination with a mineralized bone replacement graft: a report of three cases. Int J Periodontics Restorative Dent. 2010;30:139-149.
- Kao DW, Kubota A, Nevins M, Fiorellini JP. The negative effect of combining rhBMP-2 and Bio-Oss on bone formation for maxillary sinus augmentation. Int J Periodontics Restorative Dent. 2012;32:61-67.
- Froum SJ, Wallace S, Cho SC, Rosenburg E, Froum S, Schoor R, Mascarenhas P, Tarnow DP, Corby P, Elian N, Fickl S, Ricci J, Hu B, Bromage T, Khouly I. A histomorphometric comparison of Bio-Oss alone versus Bio-Oss and platelet-derived growth factor for sinus augmentation: a postsurgical assessment. Int J Periodontics Restorative Dent. 2013;33:269-79.
- Del Fabbro M, Bortolin M, Taschieri S, Weinstein RL. Effect of autologous growth factors in maxillary sinus augmentation: a systematic review. Clin Implant Dent Relat Res. 2013a;15:205-216.
- Lundgren S, Andersson S, Gualini F, Sennerby L. Bone reformation with sinus membrane elevation: a new surgical technique for maxillary sinus floor augmentation Clin Implant Dent Relat Res. 2004;6:165-73.
- Cricchio G, Palma VC, Faria PE, de Olivera JA, Lundgren S, Sennerby L, Salata LA. Histological outcomes on the development of new space-making devices for maxillary sinus floor augmentation. Clin Implant Dent Relat Res. 2011;13:224-230.
- Mazor Z, Horowitz RA, Del Corso M, Prasad HS, Rohrer MD, Dohan Ehrenfest DM. Sinus floor augmentation with simultaneous implant placement using Choukroun’s platelet-rich fibrin as the sole grafting material: a radiologic and histologic study at 6 months. J Periodontol. 2009;80:2056-2064.
