A 70-year-old woman without medical problems came to a private dental clinic to correct esthetic and functional problems. Intra-oral examination revealed collapse of vertical dimension, severely worn maxillary lower and upper cuspids and incisors, upper Kennedy class III edentulous areas. In the lower arch there were two tooth supported FDP needing replacement due to marginal infiltrations and esthetic issues . Minor signs of periodontal disease were present, with no pathologic probing depth and BOP after scaling and root planing . The patient refused any implant supported oral rehabilitation. In the preliminary stage preliminary impressions were taken, a face bow and esthetic face bow were recorded. Centric relation recording and increased vertical dimension were achieved with Beauty Pink Extra Hard wax.The obtained casts were mounted in an articulator, using the face bow, the esthetic indications from esthetic face bow and the waxes. At this moment the technician created a wax up and made four temporary posterior bridges at the chosen vertical dimension. The temporary bridges were applied in both arches after the preparation of the upper teeth and the re-preparation of old lower bridges.
Once achieved the centric occlusion and increased the vertical dimension with the insertion of temporaries posterior bridges, the upper anterior group was prepared with a mini-chanfer finishing line, whilst the lower anterior group was prepared for labial veneers. Impressions were taken and the two anteriors sextants were restored with bonded Lithium DiSilicate crowns ( upper sextant) and Lithium DiSilicate veneers (lower sextant). Rubber dam was mandatory to achieve best adhesive performances. During the waiting time for lab procedures , interim restorations with an autopolymerizable acrylic resin were pressed using a silicon mould
In the posterior regions, after the restoration of anterior areas, impressions with custom trays and polyether impression material were taken and four PFM FDP were applied, achieving occlusal stability, aesthetic and function in a mutual protection relationship with anterior regions.
Clinical Steps
Fig 0. The patient at time 0

Fig 1. Lips and smile

Fig 2, 3, 4, 5, 6. Pre-op views





Fig 7, 8. Details of worn upper and lower incisors


Fig 9, 10, 11, 12, 13. Insertion of posterior temporary resin bridges and increased vertical dimension


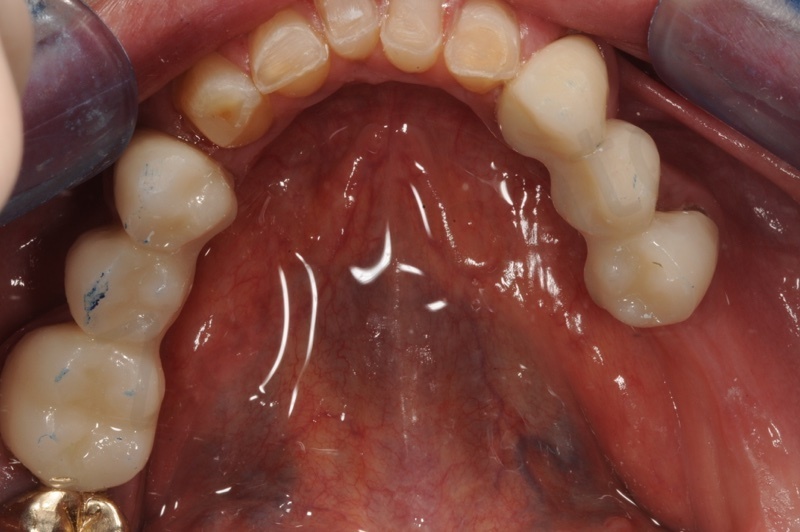


Fig 14, 15. Upper incisors prepared with the use of a silicon index


Fig 16 , 17. Anterior upper and lower sextants after preparation


Fig. 18, 19. Impressions: Custom trays and polyethers
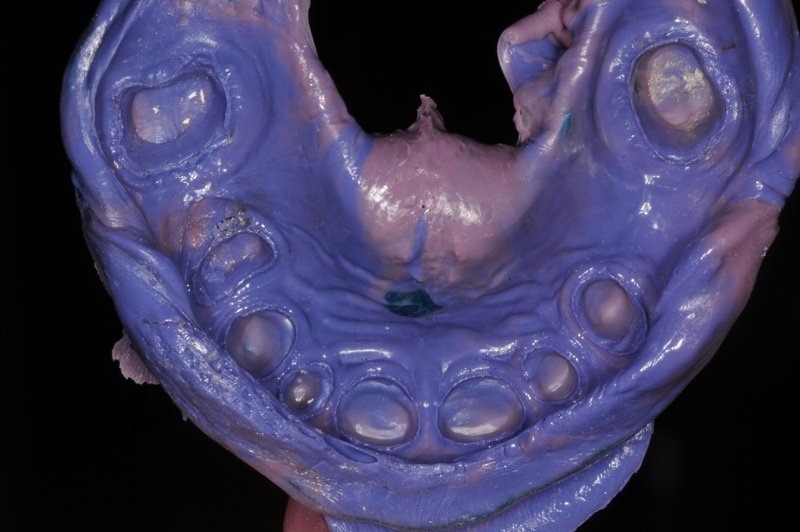
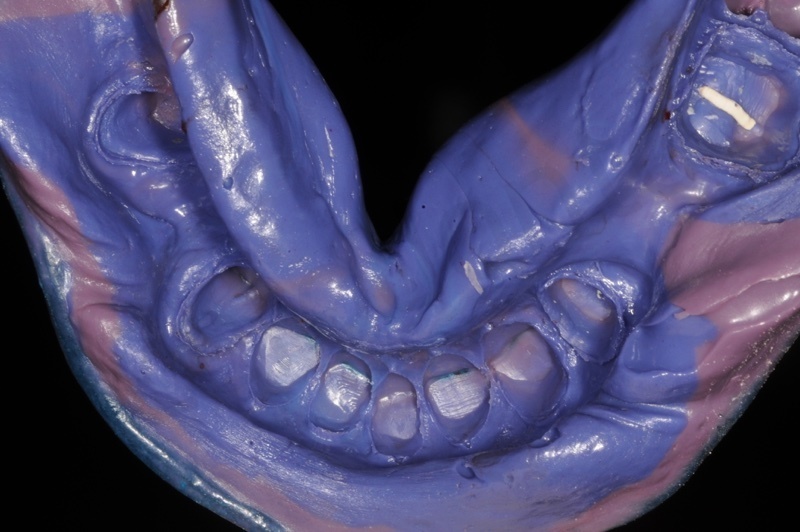
Fig 21, 22, 23. LiDiSi crowns and veneers



Fig 24, 25, 26, 27, 28, 29. Bonding procedures to ensure a reliable adhesion between dental substrates and ceramic restorations. Rubber dam is mandatory to achieve good clinical performances






Fig. 30, 31, 32, 33. Anterior sextants after bonding procedures




Fig. 34, 35. Upper and lower plaster models with die spacer

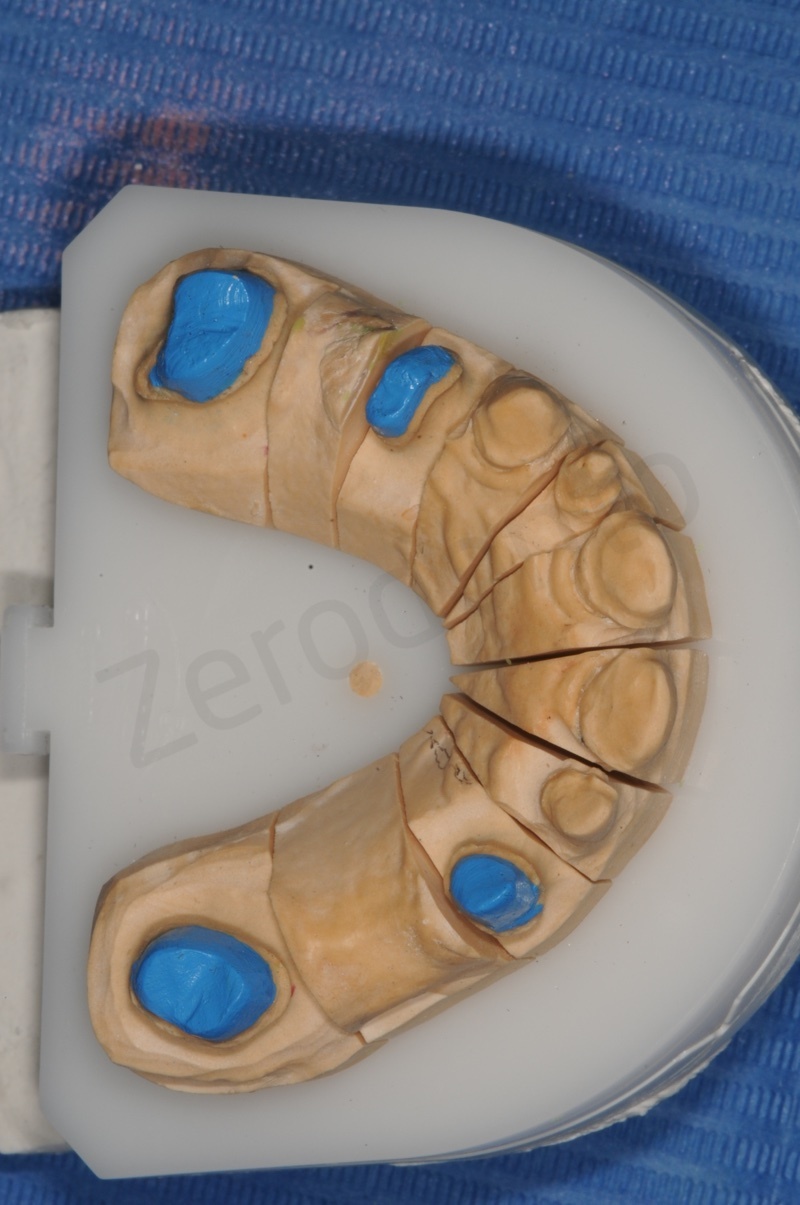
Fig. 36a, 36b. Casts in the model


Fig. 37, 38, 39. Checking castings and occlusion



Fig. 40, 41, 42, 43, 44. Baked ceramic testing



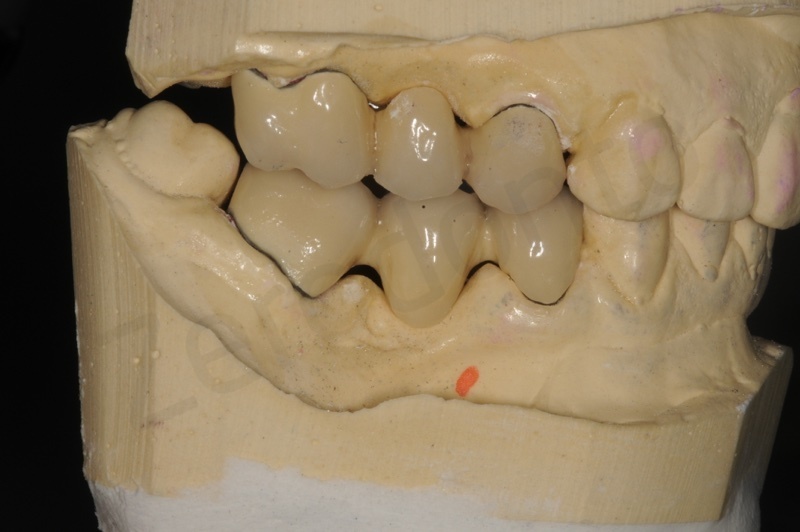

Fig. 45, 46, 47, 48, 49. Bridges completed and ready for cementation




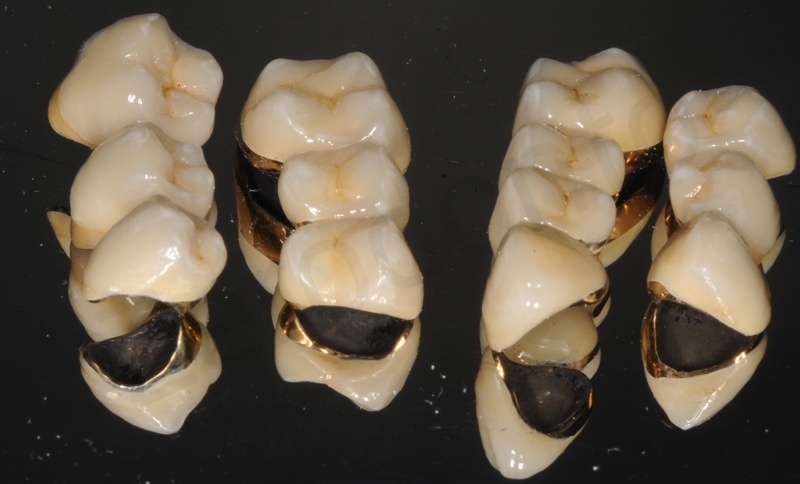
Fig. 50, 51, 52, 53,54, 55. Rehabilitation completed after luting procedures.






Fig. 56. The smile of the patient

Fig 57. Final picture of the patient and her appreciation
