Dear friends,
I’m doctor Loris Prosper a dentist and a dental technician. I love our beautiful work since I started doing it, more than 45 years ago. My area of expertise is fixed prosthodontic in aesthetic area that, in my opinion, should respect biology, preserve teeth and soft tissue health and respond to minimal invasive criteria since we make irreversible procedure when we prepare the abutment. It is only a short while I’ve published the book :”Bioestetics in the Oral Reabilitation “ Quintessence Publishing , that collects my expertise and my researches. Since the beginning of my practice my mission was to teach all the technical expertise and the tricks I’ve been acquiring through experience and mistakes.
Much contemporary literature mainly focuses on abstractions not linked to daily practice of either general either specialist dental practitioner.
From my point of view the most important thing is clinical relevance, how to perform dental procedures at best. What abutment design is the best for a particular tooth, for that gingiva, for that mouth and for that patient? What pros and cons a shoulder, a bewelled shoulder, a chamfer or a feather edge preparation do have? How much incisal, cervical and axial reduction need a specific restorative material and what finish line is best? And, even more important, how do we do that?
I’m working on a new book, an atlas, to answer these and other questions. It will be a step by step guide to tooth preparation for veneers, partial and full crowns. Each preparation on every tooth is described, and indications are given on what preparation fits better into different clinical situations: if the abutment will support a single crown or a bridge, tooth position, restorative material, periodontal health, importance in occlusal function.
Personally I find quite challenging canine full preparation. Since canine have a key role inside oral function and their prosthetic replacement is often difficult. Since the important extra-axial forces to which they are subject, particular attention must be given to obtain a solid abutment and, at the same time, to obtain enough veneering space.
For didactic purposes the preparation was splitted in two. Exploiting the integrity of the dental simulation model I prepared just the vestibular part of the tooth in order to obtain a veneer preparation, and then I proceed in the lingual part in order to perform a full-crown preparation.
Initial case, left inferior canine

first step: using a 1,2mm round bur we make guiding grooves.




All calibrated guiding grooves are realized with the same round bur until each of them is half-bur deep that is more or less 0.6mm







With regular diameter torpedo bur the vestibular aspect of the tooth is regularized to the depth of the grooves



The proximal part of the abutment has to be reduced with an extra thin torpedo bur. It is important not to damage the adjacent tooth thus we recommend to use protective interproximal metal matrix


The finish line definition starts with a rounded shoulder bur




The color code represents the three axis of the preparation related to the tridimensional morphology of the anterior teeth (Kuwata lines). The proximal aspects are reduced with an extra thin torpedo bur. At this point we realized a veneer preparation whose proximal margins are extended through the contact areas





The same rounded shoulder bur is used to realize calibrated 2mm incisal grooves that should keep the incisal inclination of 40 degrees



It is important to obtain a smooth surface, surface grinding is easily performed with a slow speed silicon carbide wheel.

Finish line definition is gently performed with a medium (blue) then with a fine grit (red) bur

Sequence of adapted silicone points to polish the preparation (use on red ring contra angle)








The abutment out of the model. Now the tooth has a veneer preparation with interproximal extension (blue). Color code:
-green-cervical area with a chamfer finish line of about 0.6-0.8mm depth
-red-central area whose axial reduction is similar to the previous one (0.6-0.8mm)
-violet-same axial reduction with incisal minimal reduction maintaining a vestibulo-lingual sloping surface thus allowing enough to dental technician for incisal ceramic stratification. The vestibular observation point shows a correctly tapered preparation to avoid undercuts. The sagittal observation point allows to identify the slightest mesial and distal concavity



Sagittal observation point: correct position of the silicon carbide wheel bur (Dura Green Shofu)for slow speed contra angle (blue ring)


Mesial distal and vestibular aspects of the preparation after color removal. The red line enhances the characteristics of the preparation: no undercuts and clear finish line in the interproximal areas. If we finish now what we have is a veneer preparation with interproximal extension and butt joint incisal edge



If it is necessary to realize a full coverage crown we need to prepare the lingual aspect of the tooth. We start again with the round 1.2mm burr performing guiding grooves half diameter depth. Using this protocol we carry on a minimal chamfer of 0.6mm width that continues in the interproximal areas at the transition points between the two chamfers: in this two critical points the finish line is maintained well defined as we can appreciate in the lateral visions




Palatal reduction is performed with a friction grip bur that needs to be used on high speed contra angle (red ring contra angle). I designed it specifically for this purpose in anterior teeth even if it can be used for quick occlusal reduction in posterior teeth and for conditioning gengiva in pontic areas. It has a wide diameter and a surface that is the negative replica of the lingual fossa of anterior teeth thus allowing omogeneous palatal reduction. Because of its shape I called it balloon bur. The red color identifies the preparation design obtained. In my opinion it is the goal in each incisive-canine preparation because it has a calibrated, conservative and homogeneous reduction



Polishing the palatal side with the same silicon points that progressively round their tip and look like the balloon bur thus helping to reach all surfaces. It is important to tilt the point in order to maximize the contact area




In order to enhance surface characteristics it is possible to use a colored powder spray commonly used for occlusal check in labs. It is useful because it makes the surface opaque and allows to point out potential undercuts. When we think the abutment is well prepared we spray the powder. Then using a polishing extra fine grit bur in reverse rotation mode (thus making impossible to damage the prepared surface) we lean for a moment the bur on the axial walls of the preparation. Undercuts are present if the line drawn by the bur doesn’t arrive till the finish line but it appears fragmented or incomplete, if it arrives undisturbed till the finish line it means that we made a good job. If undercuts are present we can remove the interfering areas without water spray using the line drawn as a guide and a fine grit bur not to exceed in dentin removal. The last two pictures shows line drawn in interproximal walls with no undercuts





Lateral point of view: an intra-operatory custom modified silicon point rounds incisal edges as all metal free preparations need no sharp edges. The two different dimensions helps reaching every part of the abutment

The same silicon point with a different shape polishing all around the preparation surface



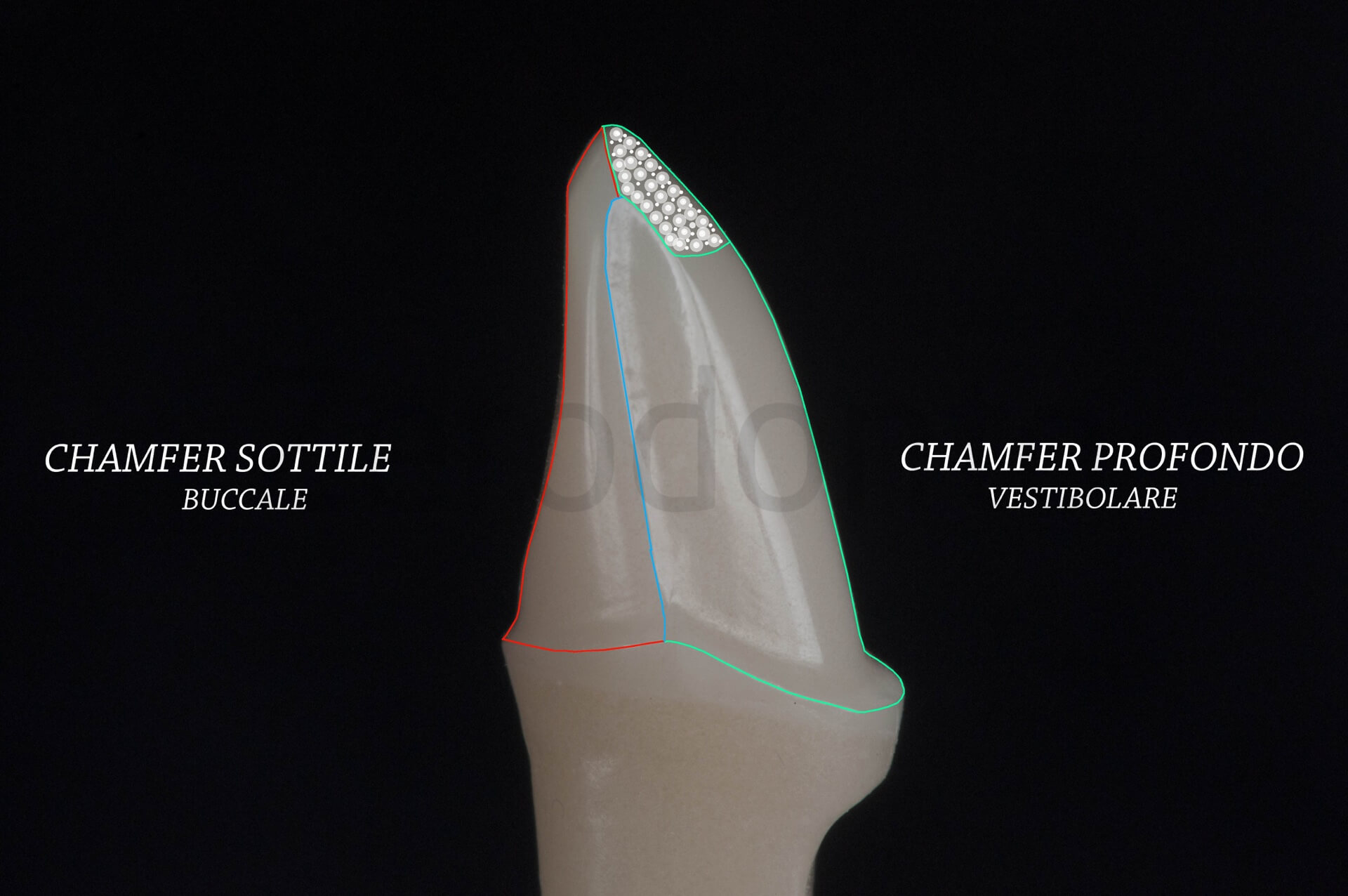
The preparation finished from different projections. The red line marks the palatal mini chamfer, the green one marks the vestibular deeper chamfer. The white incisal third needs to maintain a certain inclination to have an adequate space for ceramic stratification. The light blue line marks the transition point between lingual and vestibular preparation



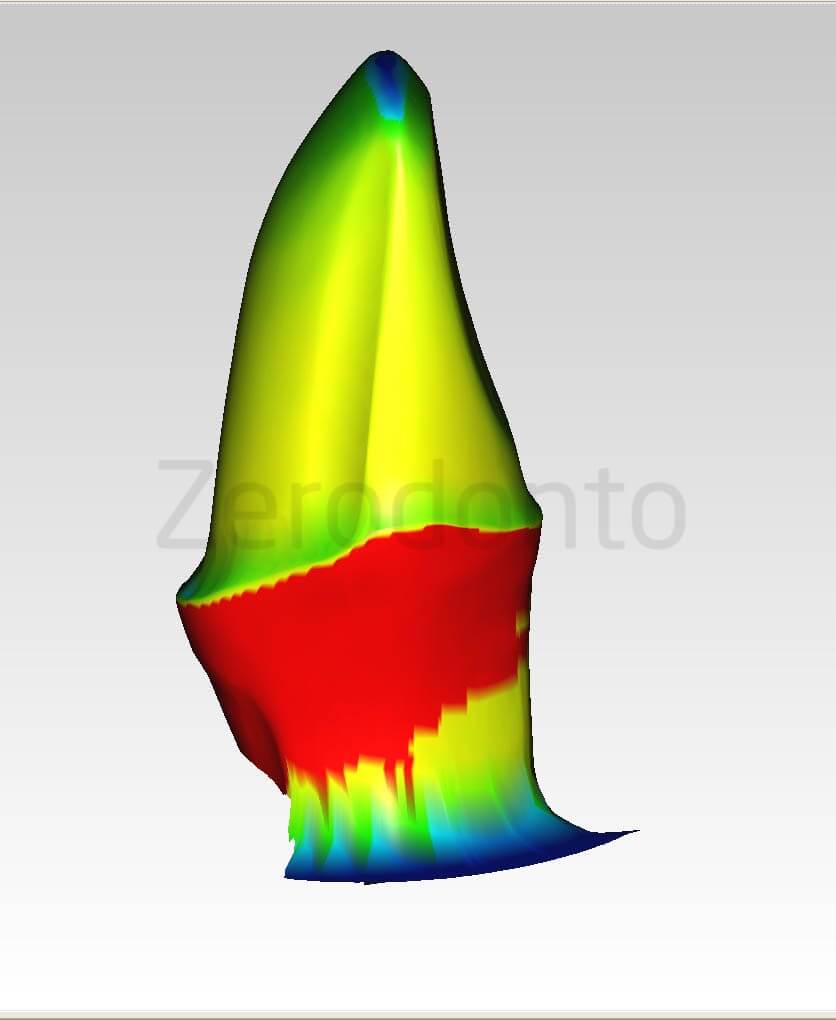
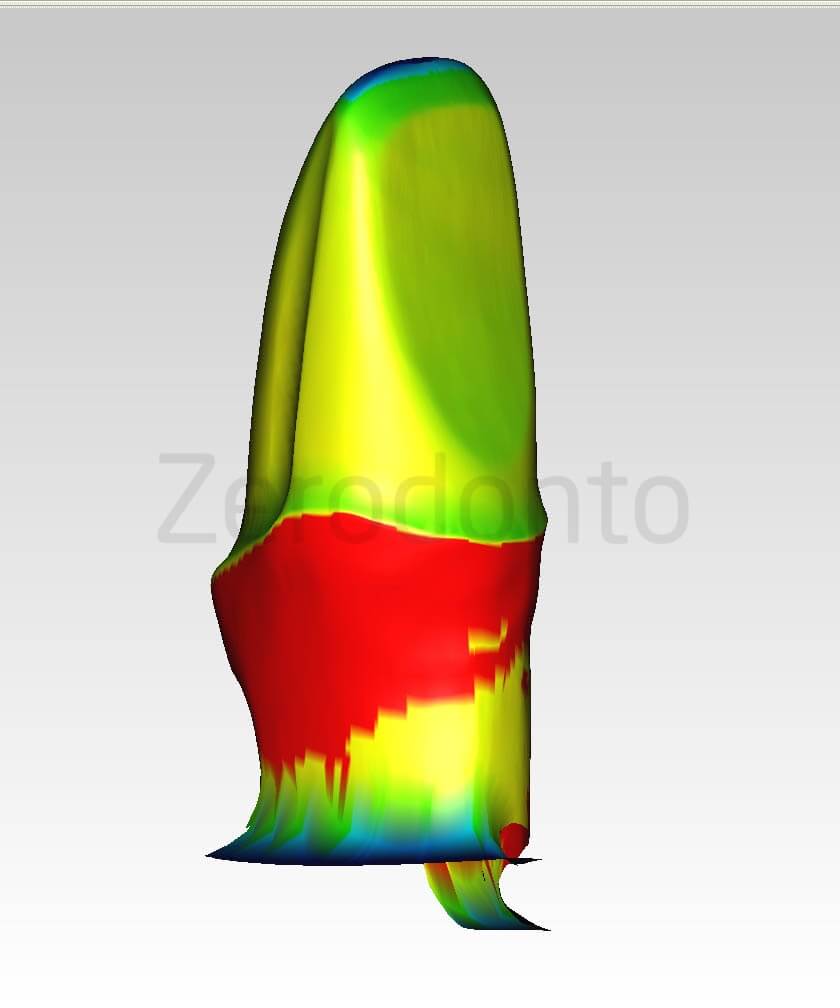
Images of the digitalized abutment. It is possible to analyze all the details and it is the litmus test for the absence of undercuts. The first image has a distal observation point, the second one is slightly rotated and has a palatal observation point. The yellow-greenish color identifies the preparation, the red one is the equal of the ditched area in the carrot model

Occlusal point of view: it possible to appreciate the different designs in the vestibular and in the lingual aspects of the abutment
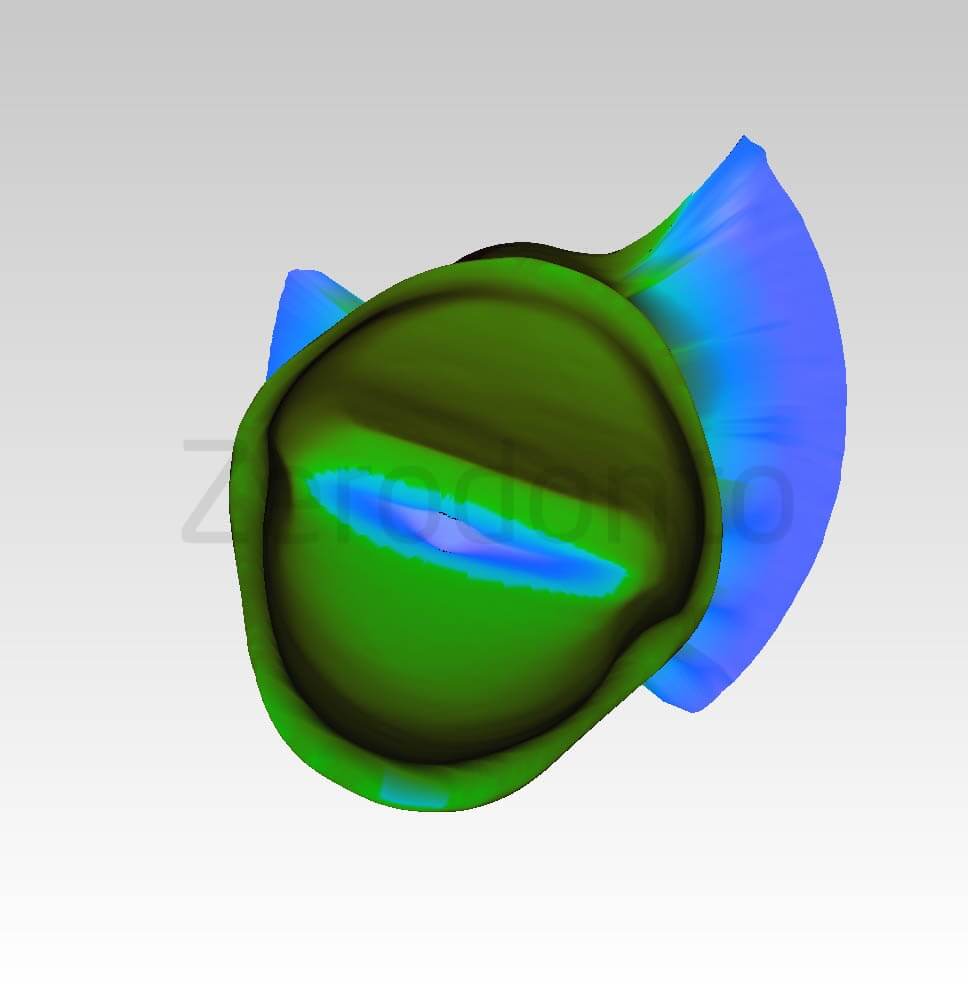
Same projection with highlighted finish line: from an occlusal point of view all finish line must be visible if not it means undercuts are present. White line marks the lingual mini-chamfer, the red line marks the vestibular deeper chamfer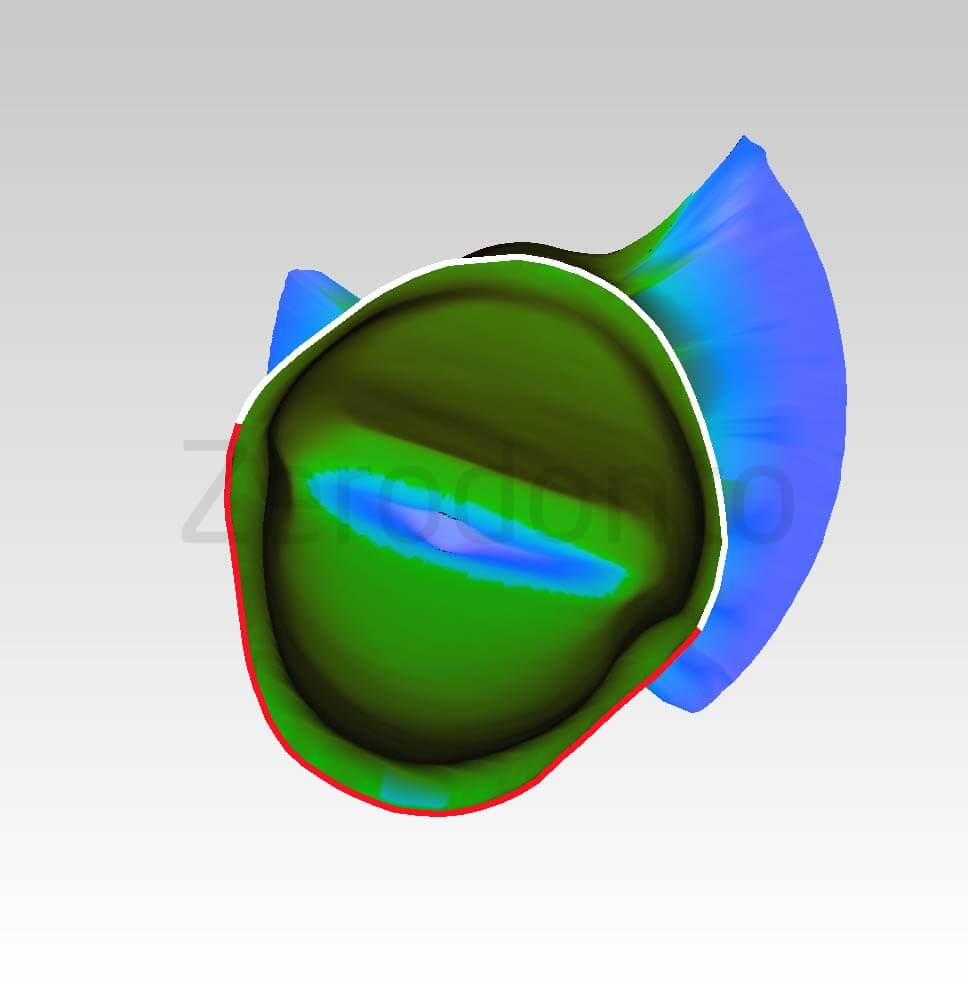
In these 3d images it is possible to appreciate the smooth transition between the different preparation designs, the red line represents the border between the two designs. There are no sharp edges.


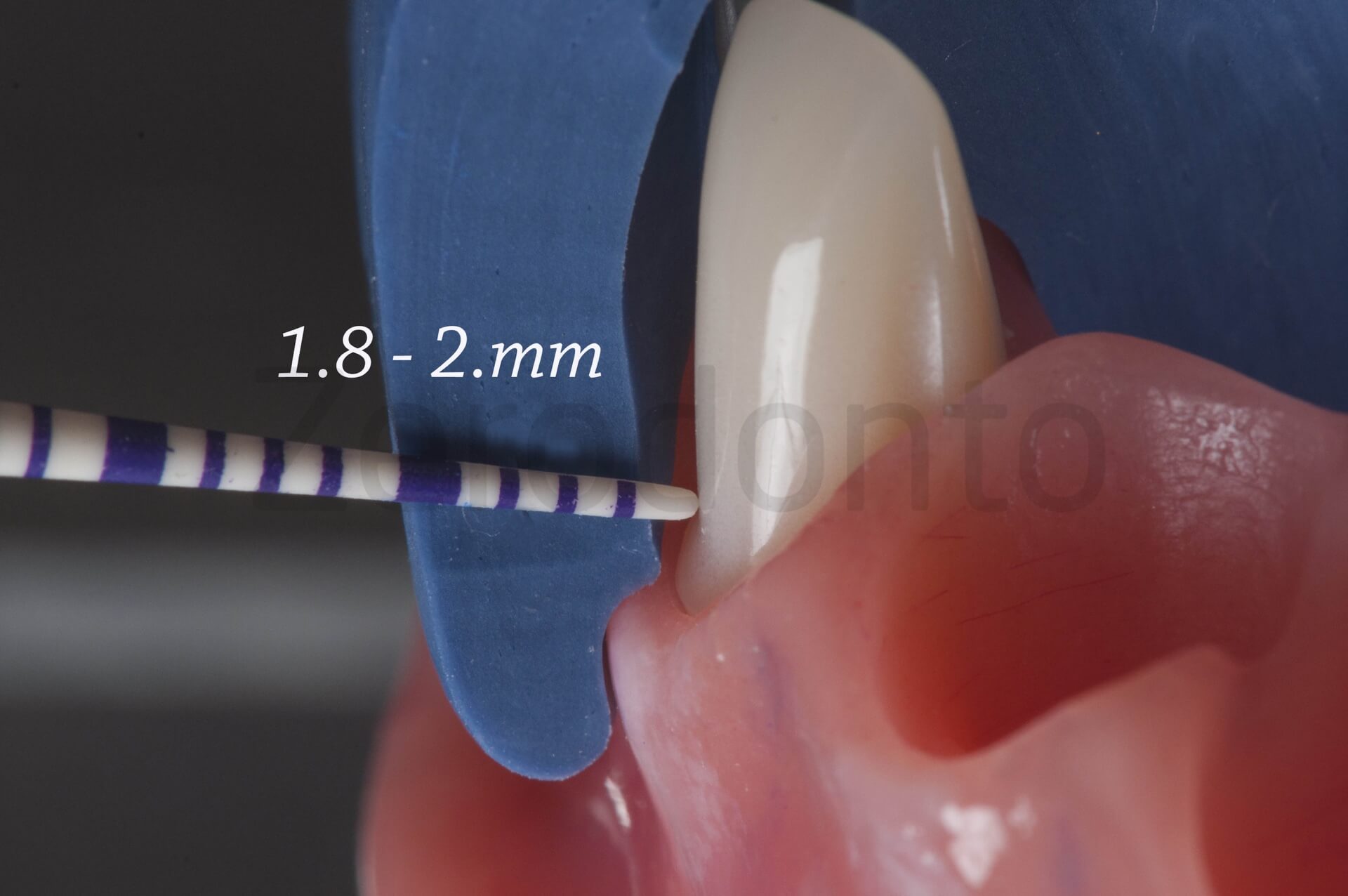
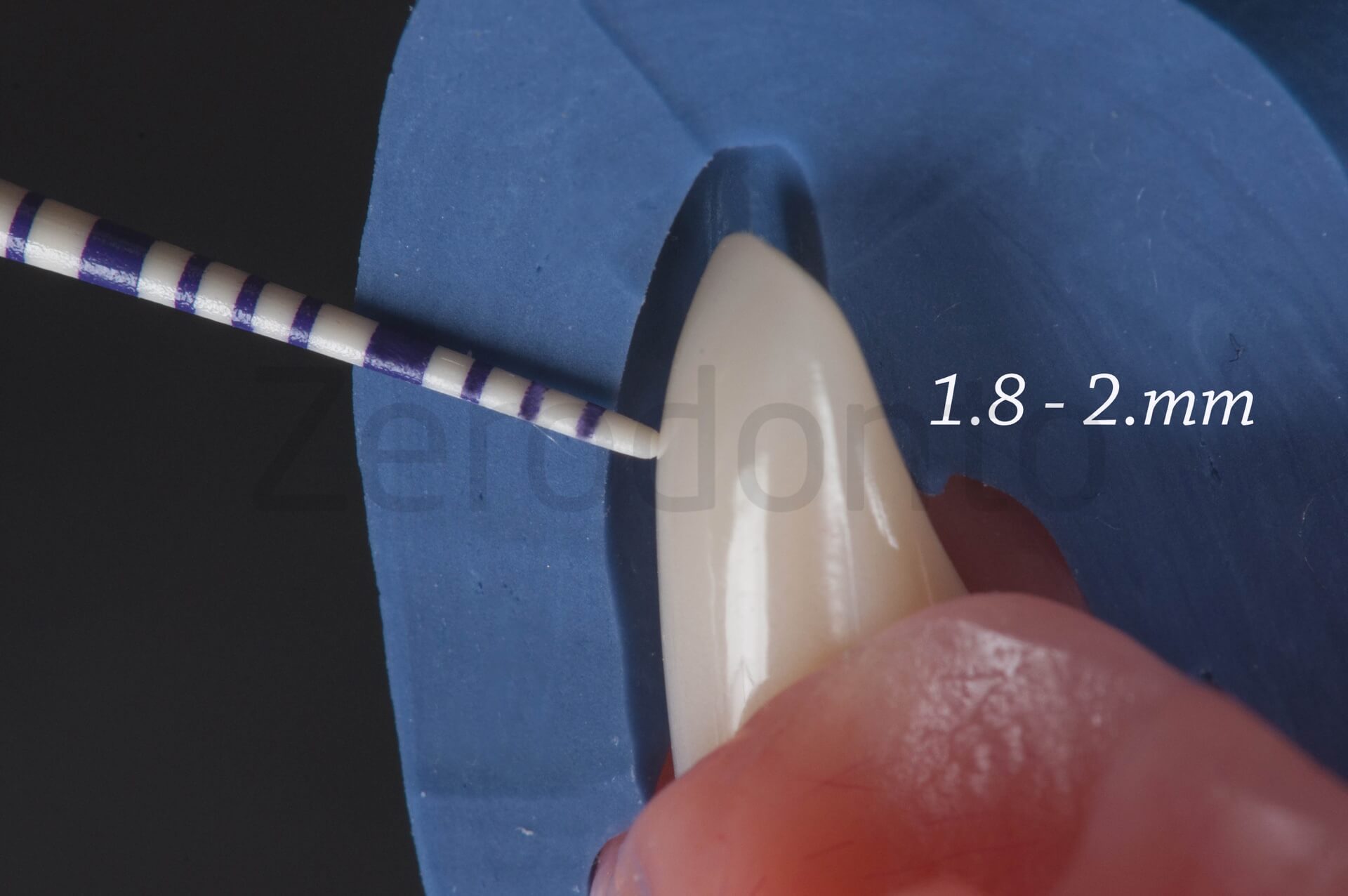
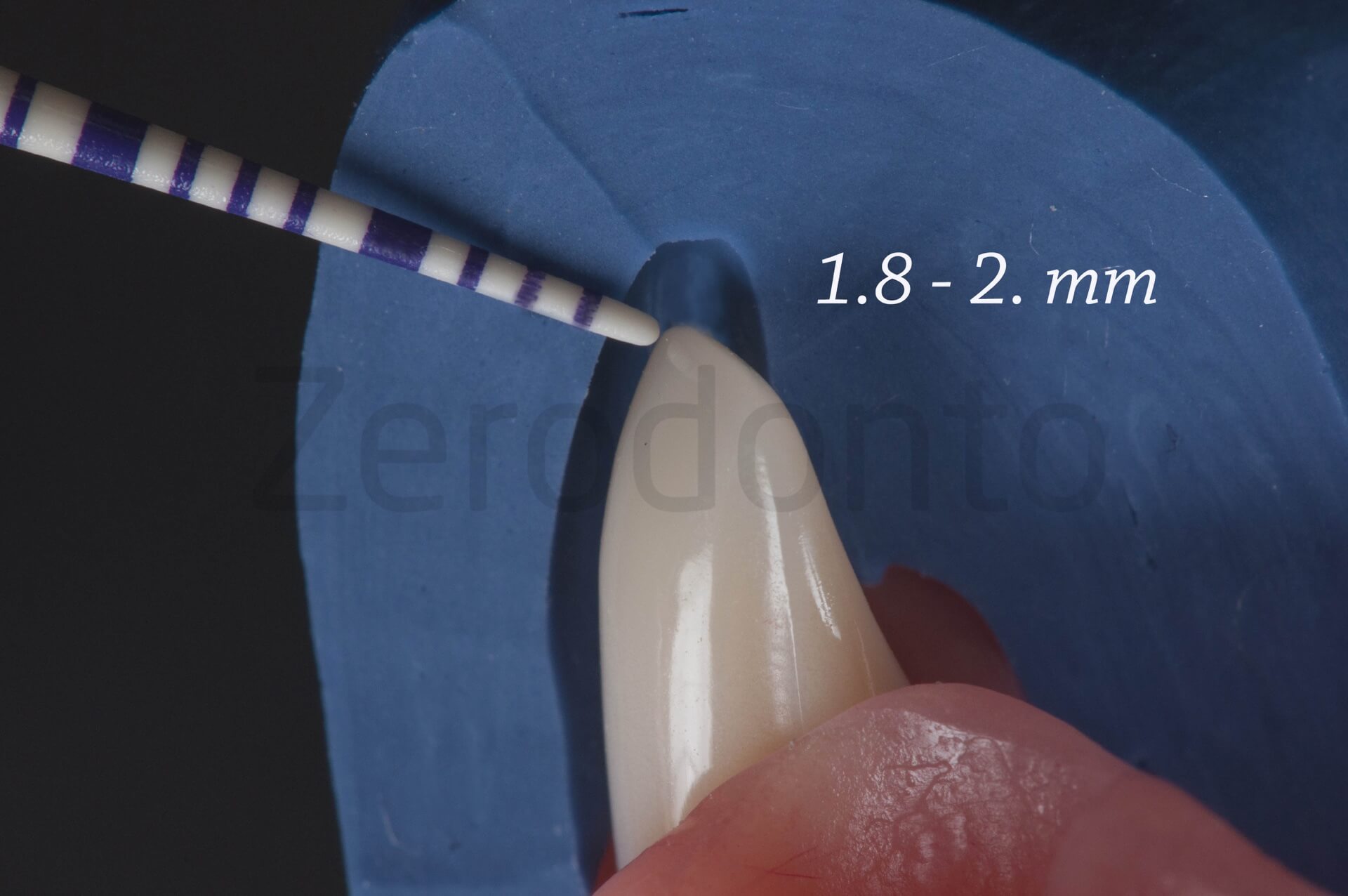
The minimum wall thickness requirements are restorative material and area dependent
cervical: 0.8-1mm
axial: 0.8-1mm
incisal: 0.8-1,5/2mm
The minimum palatal wall thickness of the crown depends on the restorative material:
ceramo-metal: 0,5mm
metal-free: 0.7 mm
Abutment impression in reversible hydrocolloid, in two different polyvinyl siloxane and in polyether respectively.


Example of a clinical case documented for 12 years of an Alumina core crown veneered with Shofu porcelain. (5l-5m) 5 year follow-up, (5n-5o) 12 year follow up












Second clinical case: 6 elements bridge, rounded bewelled shoulder preparations
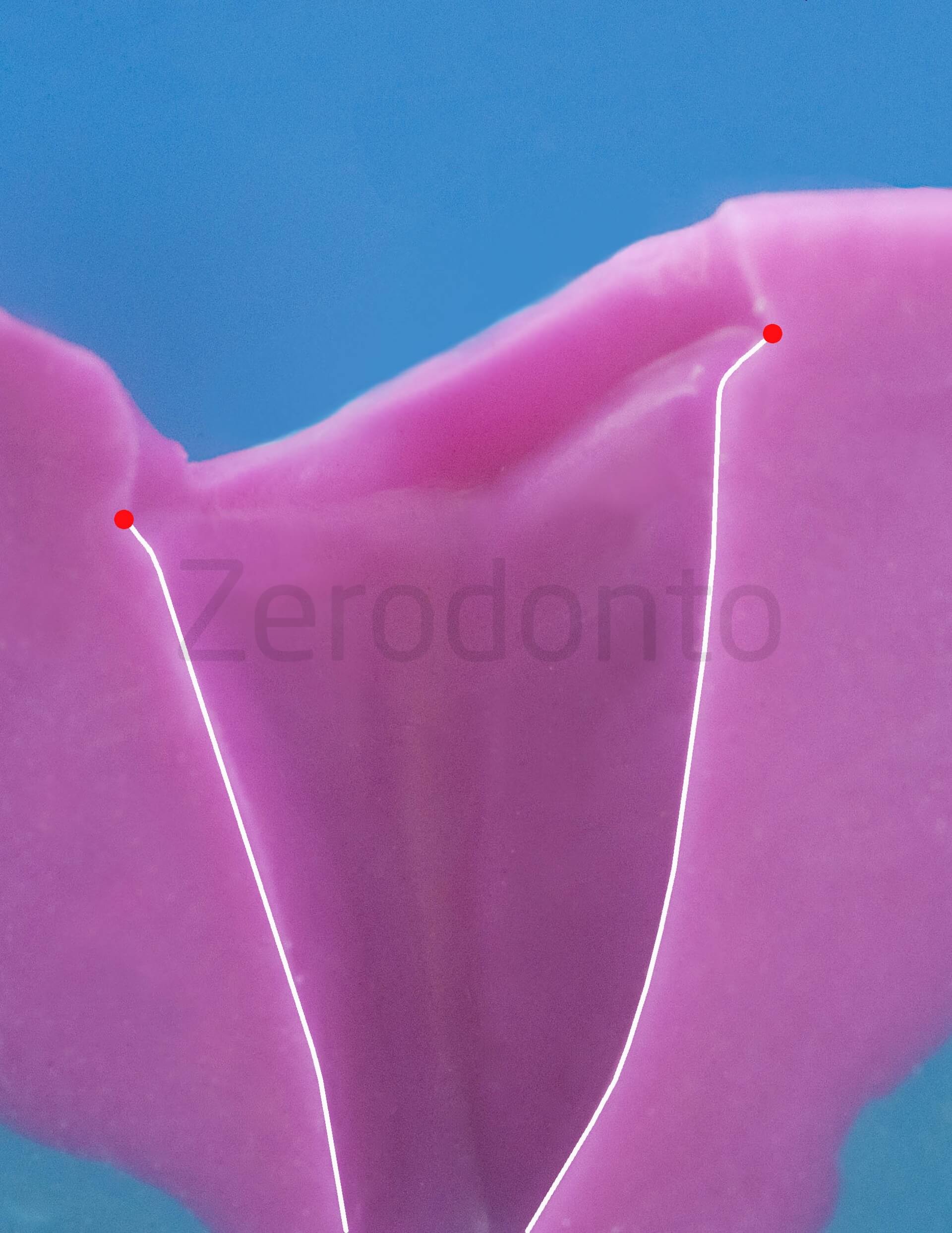
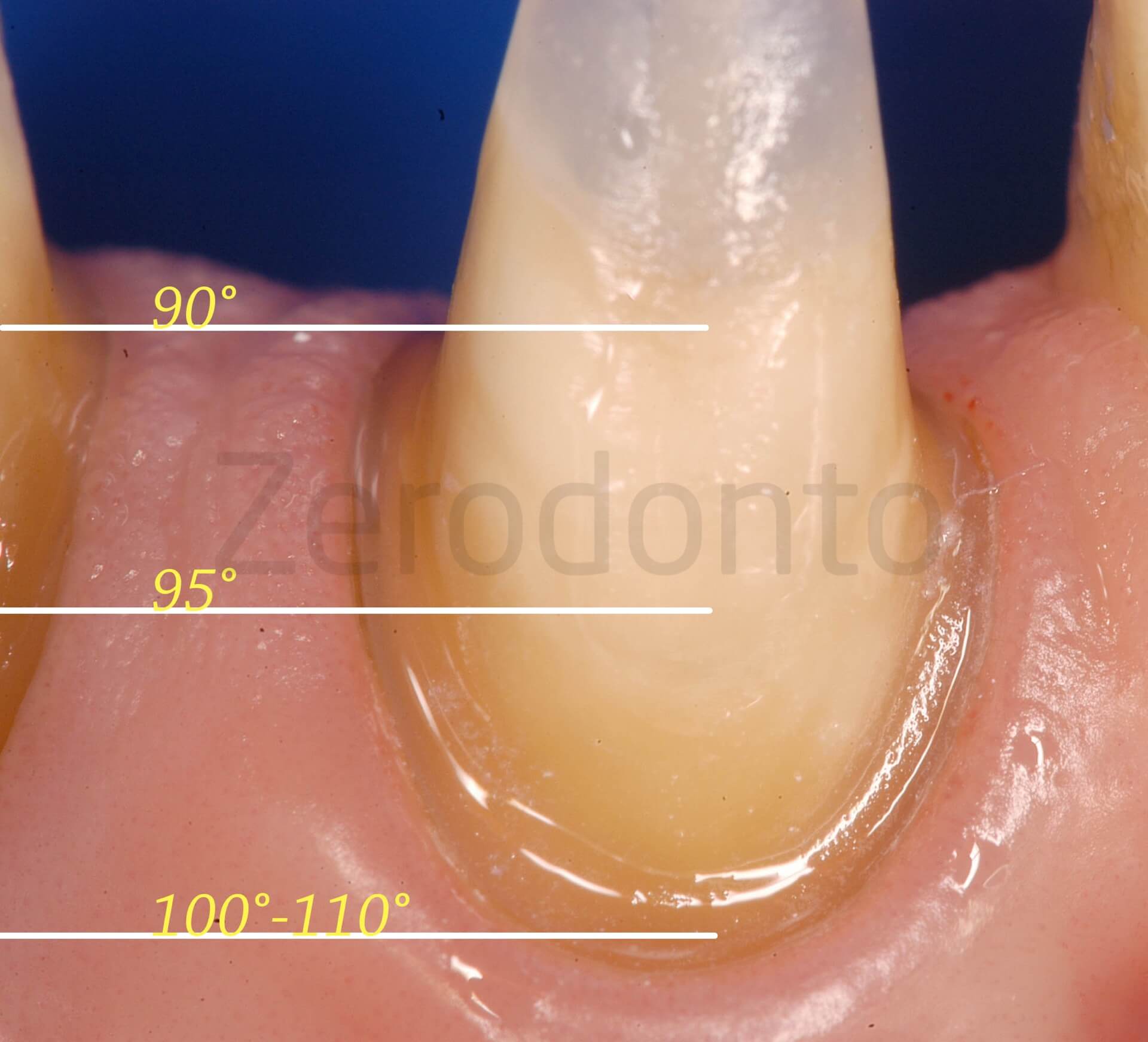
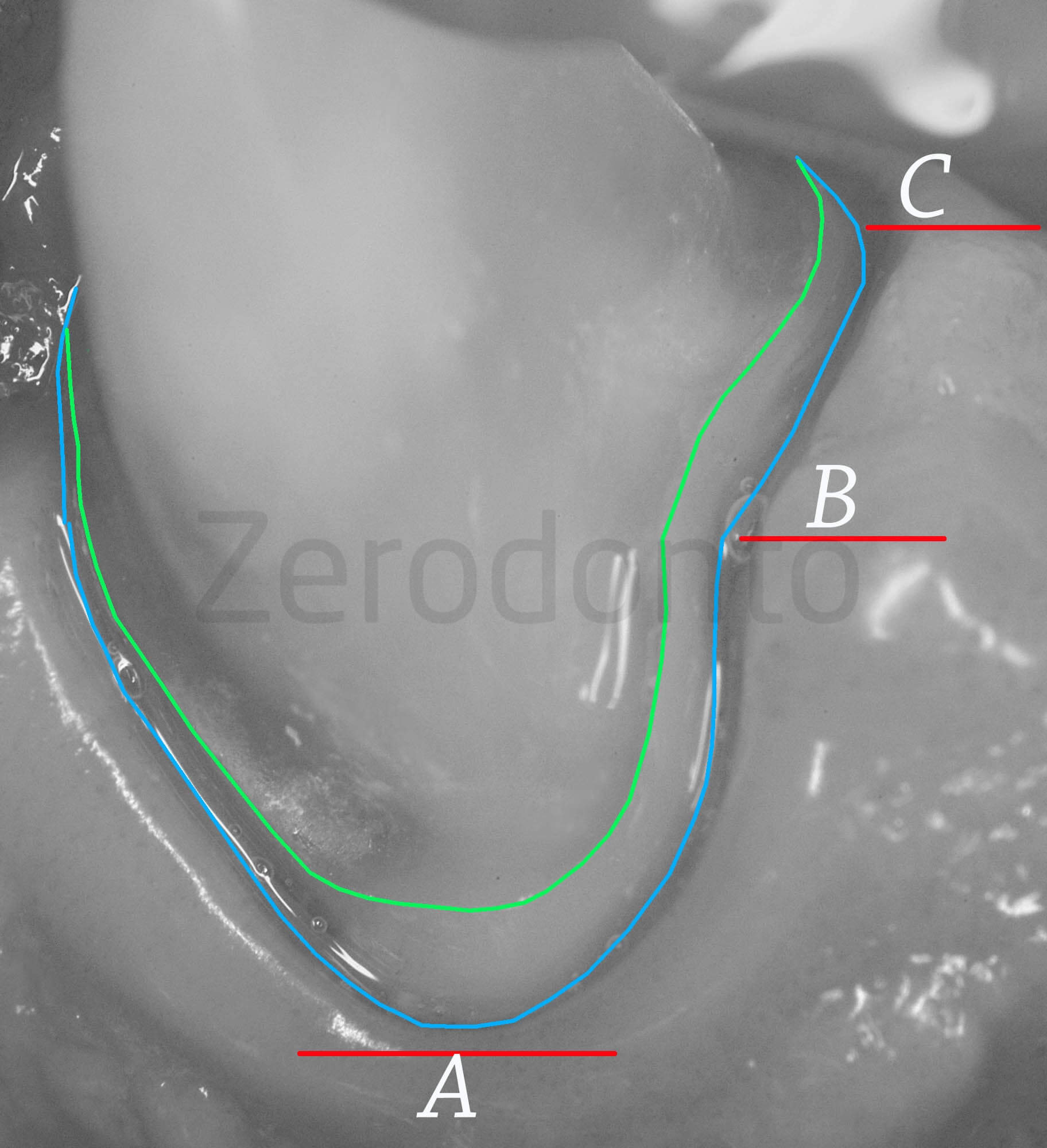
Rounded bewelled shoulder (vertical finish line) on 33 and 43. One of the most frequent adverse event that occurs in cases of complex preparations is the uncomplete seat of the crown due to premature contact localized where the finish line proceed apically from the interproximal zone to vestibular zenith. Figure 1a-b shows the three critical points of a pronounced elliptical sharp and steep shape, where the point a is far from the point B, the point B is also far from the point C.

 Polyether impression.
Polyether impression.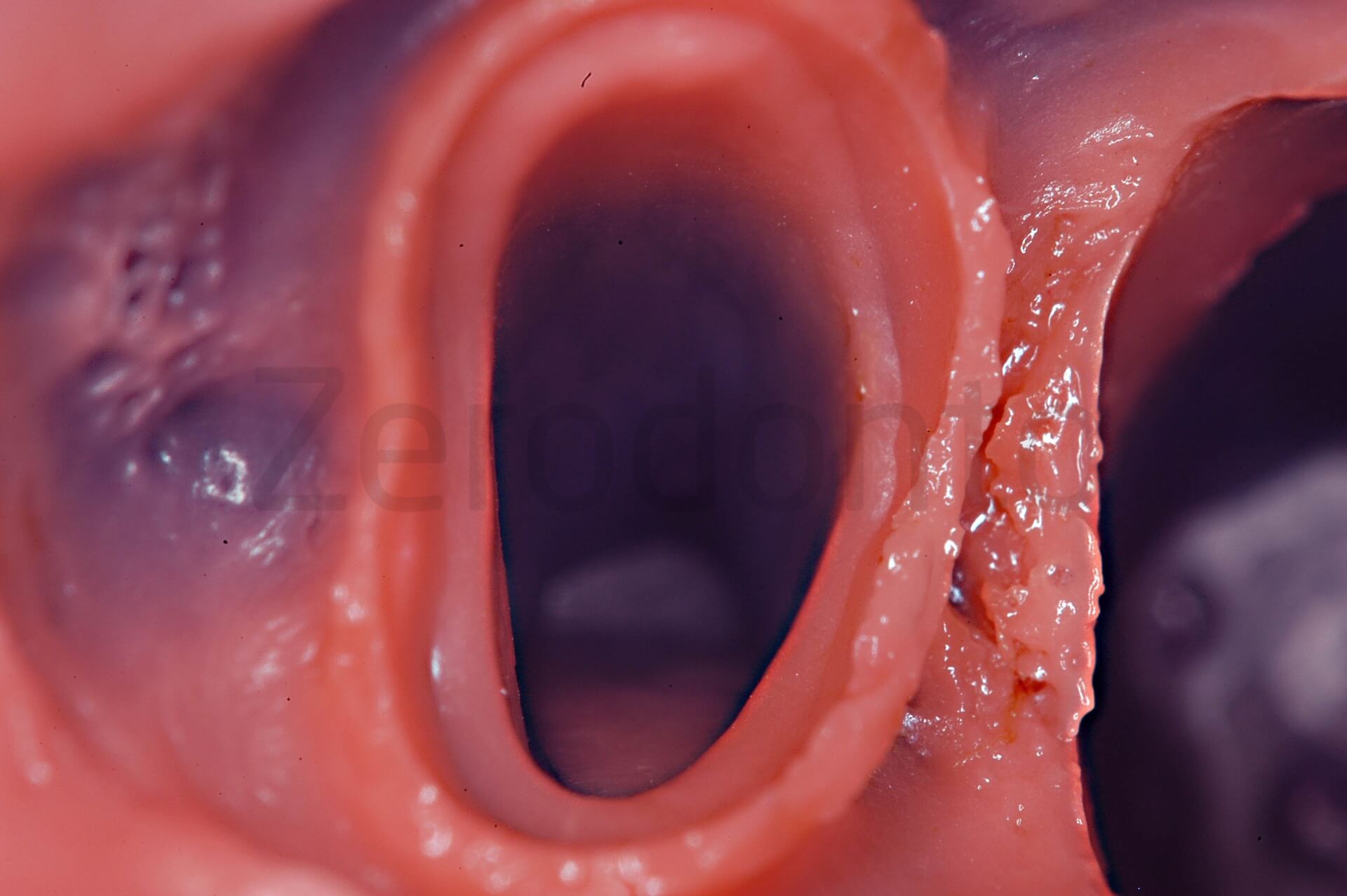


 PMMA structure try-in.
PMMA structure try-in. Final check is done with zirconium framework try-in.
Final check is done with zirconium framework try-in.

 The bridge framework was veneered using ceramic for zirconia layering (Vintage ZR Porcelain Shofu).
The bridge framework was veneered using ceramic for zirconia layering (Vintage ZR Porcelain Shofu).
Details in the inner part of the zirconia core witness compound finish line complexity. Clinical images of the cervical margins of 33 and 43 4 years after cementation, it is a clear good example of integration between the prosthesis and periodontal tissues.
Clinical images of the cervical margins of 33 and 43 4 years after cementation, it is a clear good example of integration between the prosthesis and periodontal tissues.

 Clinical cases from the book “Bioaesthetic in oral rehabilitation” Loris Prosper, Quintessence Publishing 2016).
Clinical cases from the book “Bioaesthetic in oral rehabilitation” Loris Prosper, Quintessence Publishing 2016).
