ERE (Edentulous Ridge Expansion) TECHNIQUE IN TWO STAGES.
In implant-supported prosthodontics there is often the need to insert implants with shapes and dimensions adequate to the teeth to be replaced, in line with the load forces and allowing the creation of an ideal emergence profile of the crowns.
These issues often force the surgeon to expand the remaining bone crest using procedures aiming at that goal. Among all the known “augmentation techniques”, a recent revision of scientific literature indicates the split-crest as one of the most highly predictable surgical methods, with a success rate of 98-100% (Chiapasco 2006) and the lowest occurrence of volumetric shrinkage during and after healing. In the case under examination, the splitcrested technique – to be more specific the ERE (Edentolous Ridge Expansion) (Bruschi and Scipioni) – was used; the surgical protocol of this technique of ridge expansion requires a partial thickness flap, not to cause cortical bone periosteum loss.
The tissue is subsequently repositioned apically; both the gingival wound and the mineralized tissue are made heal for second intention. The implant was made transmucosal by inserting the healing abutment in the surgical phase. When one faces a particularly thin ridge with little marrow or a not very elastic bone, difficult to distract, it is better to adopt the two-stage technique, allowing 40/50 days between the two operations. It is well known that in the first stage of its healing process, the bone goes through its osteoclastic phase of healing, losing part of its mineralized component and making the tissue structure much more elastic (woven bone): this feature makes it much easier to distract it.
Following the protocol, to execute the primary sagittal and release incisions – needed to plan release lines of the bone walls to distract – there is a wide choice of instruments that can be used: manual, rotary, reciprocating, piezoelectric, etc.
The latest instrument coming out for this purpose uses the micro-vibrating sonic movement of air-driven handpieces (e.g. Sonicflex kavo). Sonosurgery bonetips “sonic” instruments are made by Komet (Gebr. Basseler DE): they come in 3 shapes that are well suited to reach any place of possible operation within the mouth, even the most inaccessible. One of the most important features of these tips is to have a very thin incision section (0.2 mm), impossible to obtain with other known instruments used for this purpose, not even the piezosurgical ones.
This feature allows to spare precious bone and, at the same time, does not cause heating; as a matter of fact, the small metal mass of the blades limits the building up of heat, which is immediately dissipated. Moreover these instruments have a bone tissue selective cutting feature and ensure the most absolute respect to the integrity of soft tissues: this is due to the slow movement, compared to other instruments, but especially because there is no need to exert pressure during the use.
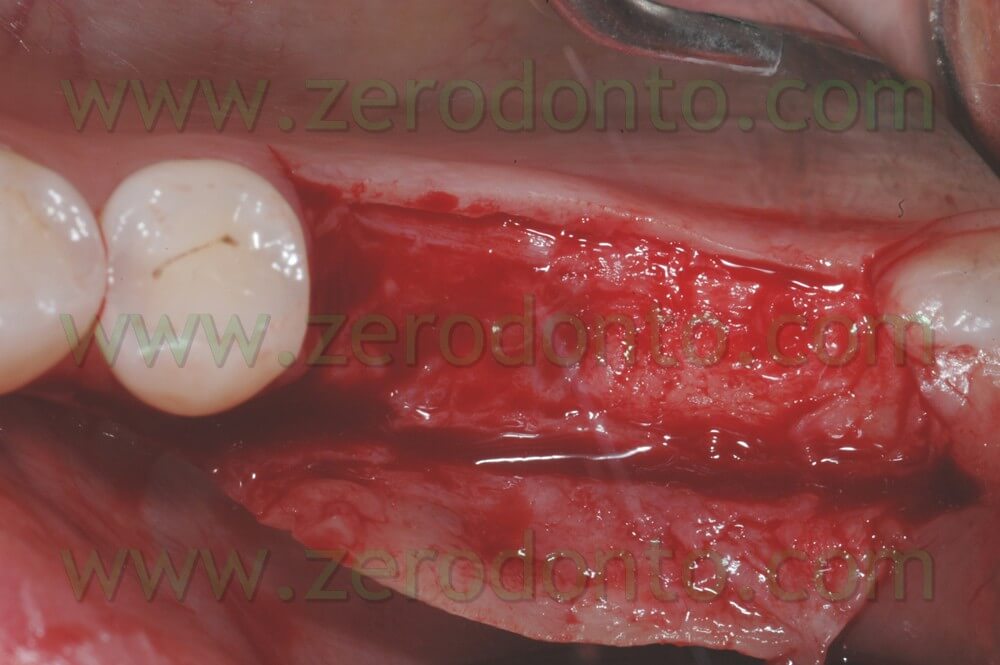
Picture 1: Initial condition of the mandibular right edentulous saddle.

Picture 2: Incision and elevation of the partial thickness flap without exposing the bone.
Picture 3: Sonosurgery instrument with coplanar blade, in position to start the sagittal incision of the ridge.
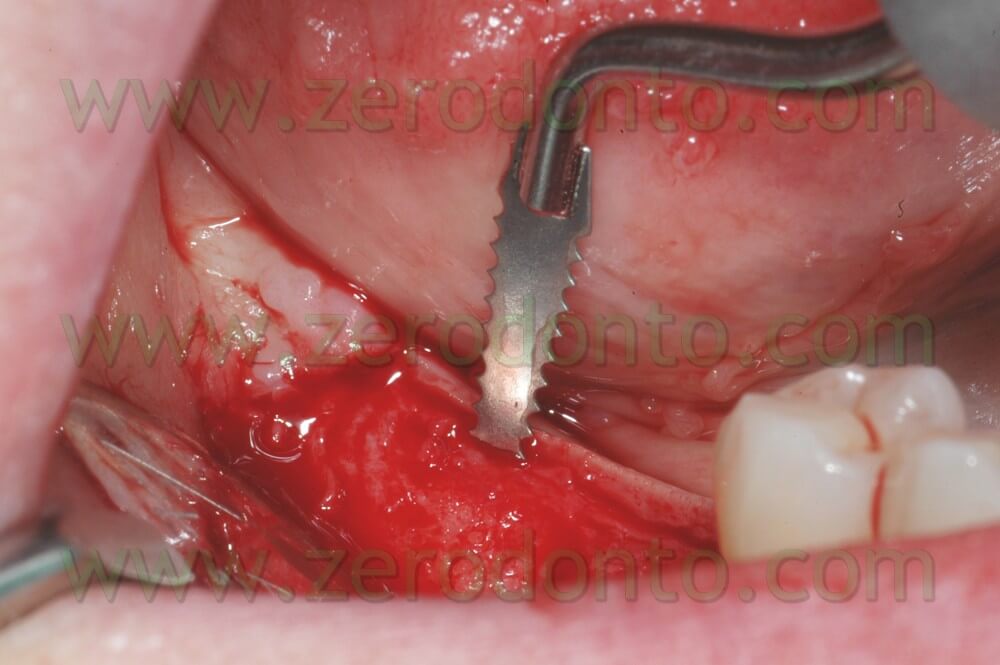
Picture 4: The instrument is totally sunk for 10 mm into the bone

Picture 5: Beginning of the distal release incision with orthogonal blade, allowing to make a 90° incision, with respect to the previous one, keeping the same orientation of the handpiece.
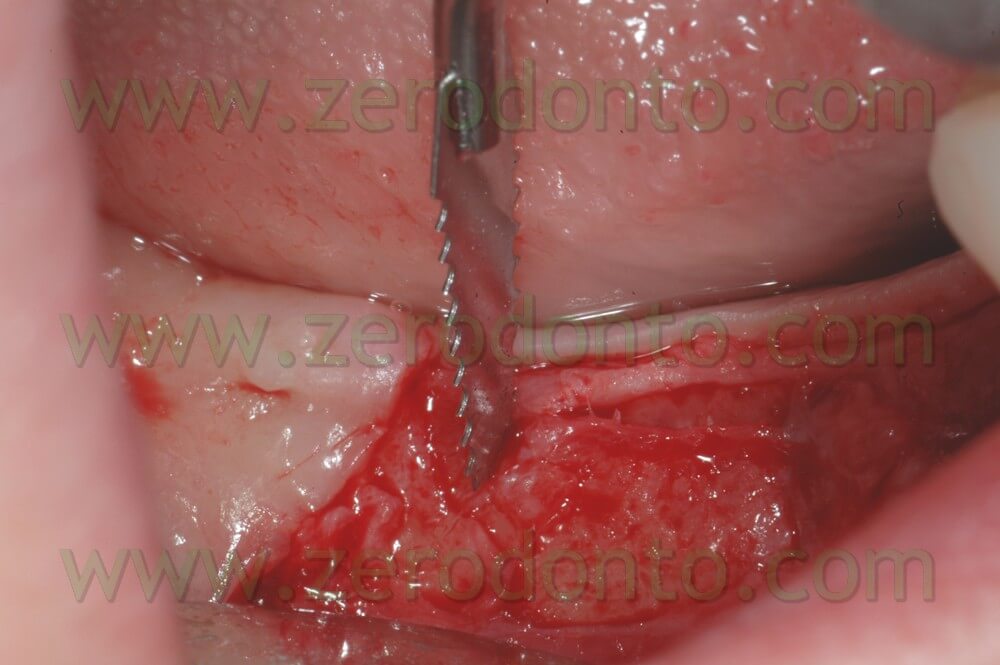
Picture 6: Extension phase of the distal bone release.

Picture 7: Mesial bone release incision, performed with the orthogonal tip; in case there is hindrance to the shank of the instrument by nearby dental elements, it is useful to use the straight tip to solve the problem.

Picture 8: View of the ridge with the distraction programming primary incisions, performed through the connective tissue previously cut with the scalpel: the use of the scalpel was necessary because of the impossibility for sonic instruments to cut soft tissues.

Picture 9: First limited ridge expansion that does not make it possible to insert adequate implants: the bone flap is kept distracted by titanium wedges (Sweden e Martina) till the second surgical phase.

Picture 10: Situation 6 days after removing the sutures.

Picture 11: Same date after removing the sutures: notice the volume increase of the ridge.

Picture 12: View of the healing tissues 40 days after the first operation.

Picture 13: The ridge after removing the titanium wedges and an expansion test to try out the bone density: being demineralized it is easier to shape.

Picture 14: After inserting the implants and the healing abutments, the flap was repositioned apically and sutured with subperiostal detached stitches in order to increase the volume and the keratinized gum band.

Picture 15: The sutures are removed after 6 days: notice the gap filled by fibrin; letting it heal for second intention will result in new keratinized mucosa and new bone.

Picture 16: After about 40-50 days, when the fixing integration is over, it is time for the prosthetic phase; AMA (Dr. Calesani’s anatomically modified abutments) stump technique and interceptive impression with burred abutments.

Picture 17: AMA abutments with 0° burring, positioned within the mouth, buccal view.

Picture 18: Same situation seen occlusally.

Picture 19: Another angle to appreciate the finishing lines and the quality of the tissues.

Picture 20: Picture of the artefact in place after some weeks of use; there is a noticeable tissue integration, i.e. the quality and amount of keratinized gum around the crowns and the initial formation of papillae.

Pictures 21, 22, 23: X-rays during and after operation.



Sonosurgery Komet instruments, put on a Sonicflex handpiece, used for the operation: the coplanar is usually recommended for sagittal incisions, the orthogonal for vertical release incisions, the straight is very versatile and can be used in those cases when, either for an hindrance or an angle, it is not possible to use the previous shapes.



Bibliography:
A two-stage full-arch ridge expansion technique: review of the literature and clinical guidelines
Elian N, Jalbout Z, Ehnrlich B, Classi A, Al-Kahtani F, Froum S, Tarnow DP. Implant Dent. 2008 Mar;17(1):16-23
A 10-years multicenter retrospective clinical study of 1715 implants with the edentulous ridge expansion technique
Bravi F, Bruschi GB, Ferrini F.
Int J Periodontics restorative Dent. 2007 Dec;27(6):557-
Triple immediate therapy (ridge expansion, soft tissue augmentation, and provisional restoration) of maxillary anterior single implant.
Lay YL, Chou IC,Liaw IC, Chen HL, Lin YC, Lee SY.
J. Periodontol. 2007 Jul;78(7):1348-53
Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants.
Chiapasco M, Zaniboni M, Boisco M.
Clin Oral Implants Res. 2006 Oct;17Suppl 2:136-59.
Preliminary report on a staged ridge splitting technique for implant placement in the mandible: a technical note.
Enislidis G, Wittwer G, Ewers R.
Int J Maxillofac Implants. 2006 May-Jun;21(3):445-9.
Dental implants placed in expanded narrow edentulous ridges with the Extension Crest device. A 1-3-year multicenter follow-up study.
Chiapasco M, Ferrini F, Casentini P, Accardi S, Zaniboni M.
Clin Oral Implants Res. 2006 Jun;17(3):265-72.
Clinical application of maxillary endossenous implant with edentulous ridge expansion technique.
Huang Y, Ou Y, Song G.Hua Xi Kou Qiang Yi XueZaZhi. 2003 Oct;21(5):374-6, 388.
Piezoelectric surgery in implantology: a case report-a new piezoelectric ridge expansion technique. Vercellotti T.
Int J Periodontics Restorative Dent. 2000 Aug;20(4):358-65.
Bone regeneration in the edentulous ridge expansion technique: histologic and ultrastructural study of 20 clinical cases.
Scipioni A, Bruschi GB, Calesini G, Bruschi E, De Martino C.
IntJ Periodontics Restorative Dent. 1999 Jun;19(3):269-77.
Healing at implants with and without primary bone contact. An experimental study in dogs.
Scipioni A, Bruschi GB, Giargia M, Berglundh T, Lindhe
J.Clin Oral Implants Res. 1997 Feb;8(1):39-47.
The edentulous ridge expansion technique: a five-year study.
Scipioni A, Bruschi GB, Calesini G.
Int J Periodontics Restorative Dent. 1994 Oct;14(5):451-9.
L’improntaintercettiva in implantoprotesi: presentazione di una procedura clinica originale.
Calesini G, Bruschi GB, Scipioni A, Micarelli C.
Teamwork anno V;268-275:Apr. 2003
Abutments Modificati Anatomicamente (A.M.A.)
Calesini G, Bruschi GB, Scipioni A, Micarelli C, Di Felice A.
Quintessence International 5/6 1997
