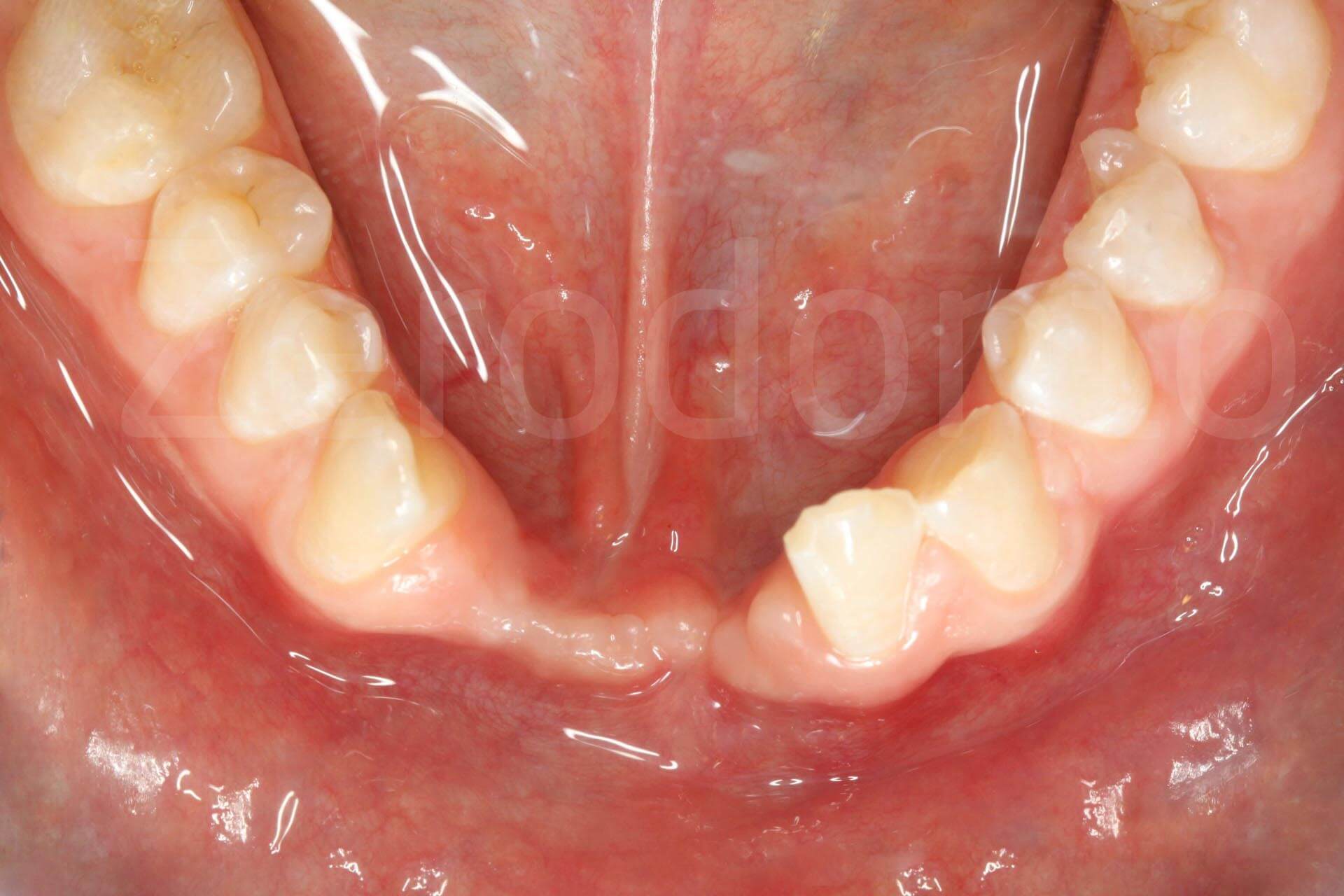
A serious car accident caused severe damage, both systemically as well as to the oral cavity of a young 17 year old female (Fig. 1).
The loss of teeth, hard tissue and soft tissue in the fifth sextant resulted in a critical esthetic-functional deficit.
The patient’s request was to restore the compromised zone with a prosthetic rehabilitation that would be as similar as possible to the area prior to the trauma, avoiding solutions that foresee the presence of artificial gingiva .
The required vertical bone regeneration exemplifies one of the most complex procedures, mainly with regards to the correct management of the soft tissue compromised by the injury.
Following an accurate clinical-radiographic assessment of the skeletal maturity, a complex therapeutic strategy was undertaken (Figs. 2, 3).
Fig. 1. Complex rehabilitation of the esthetic area: initial phase
Extraoral view and details of the smile.


Intraoral images a few months after the trauma.

Orthopantomography and latero-lateral X-ray.
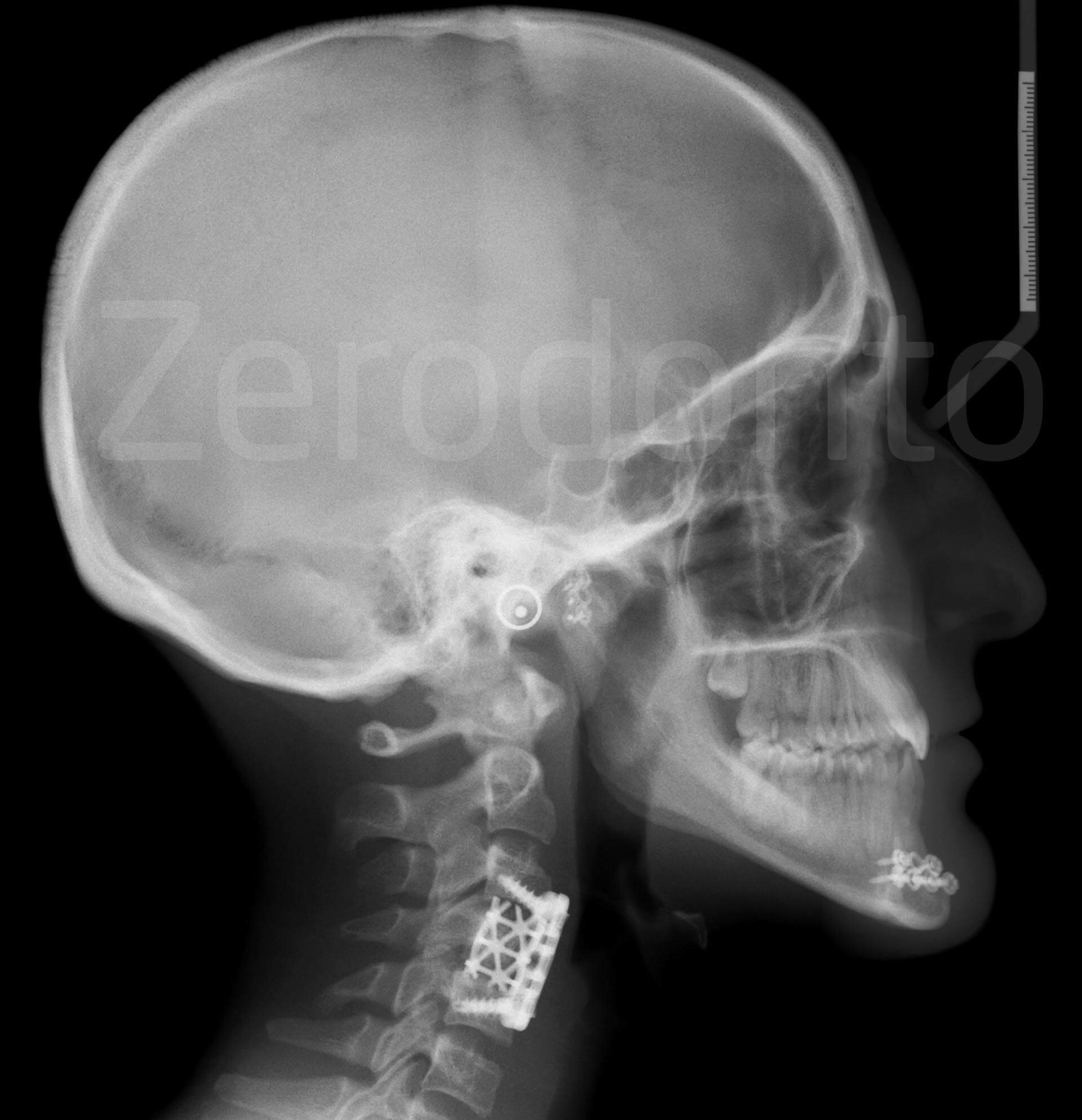
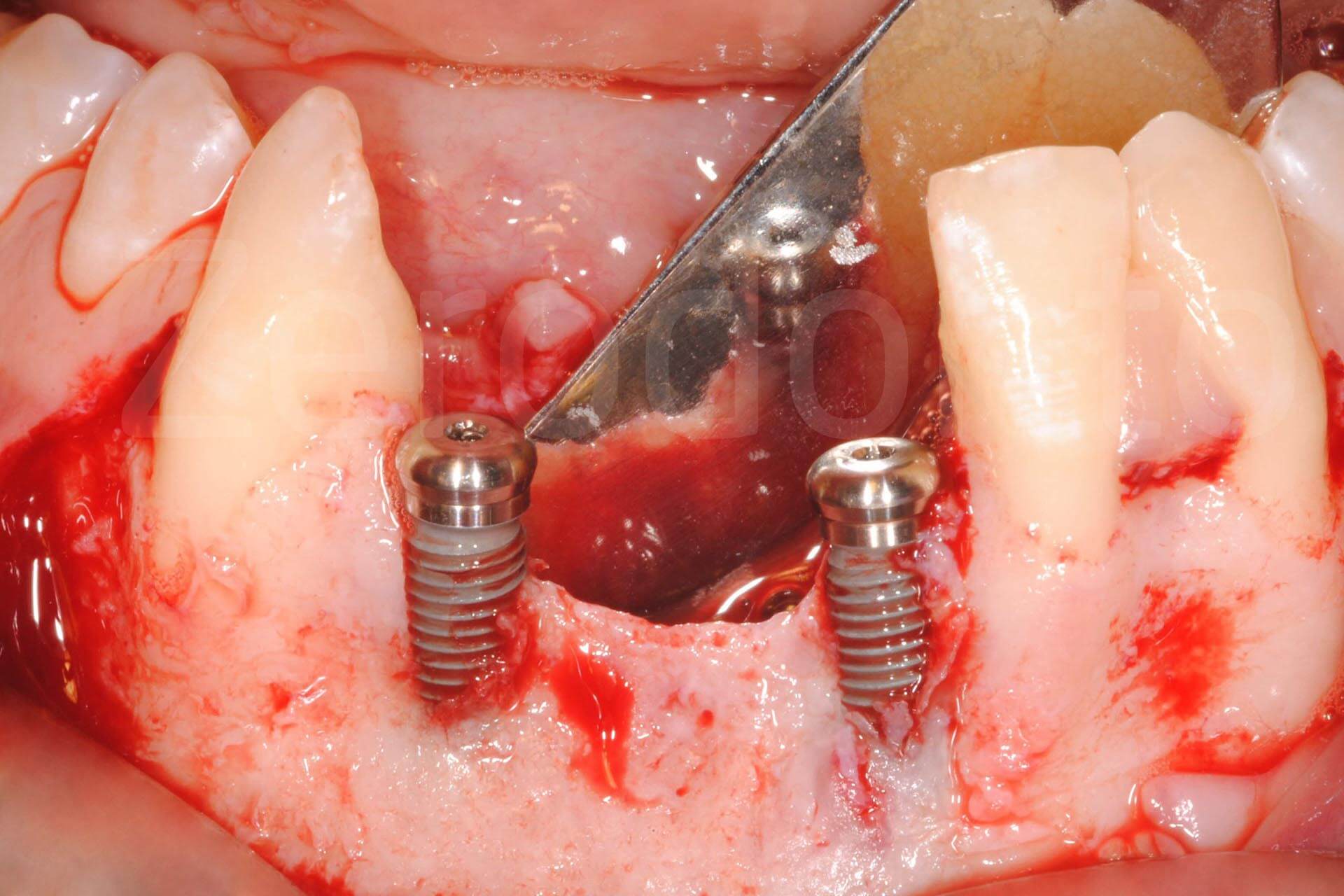
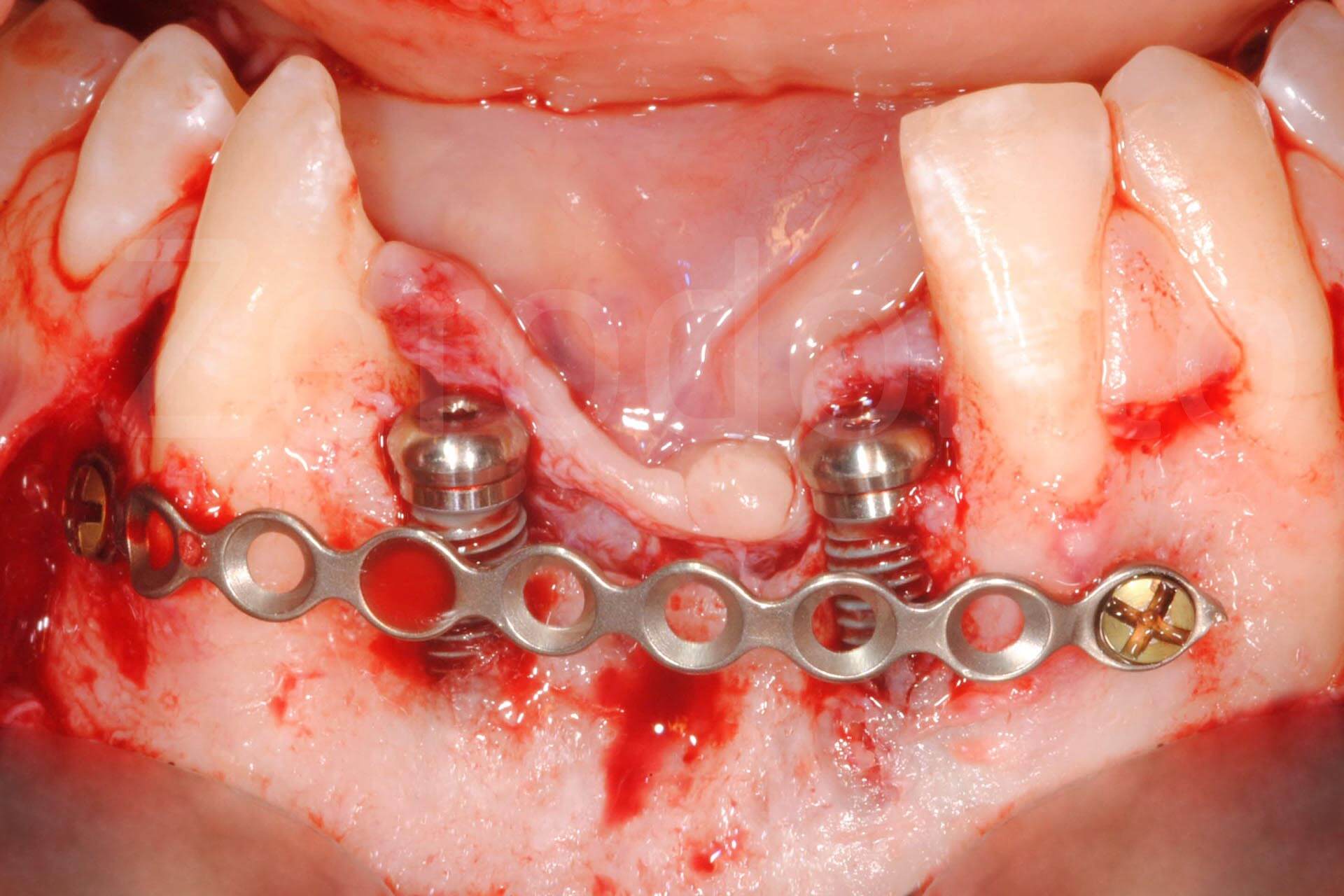
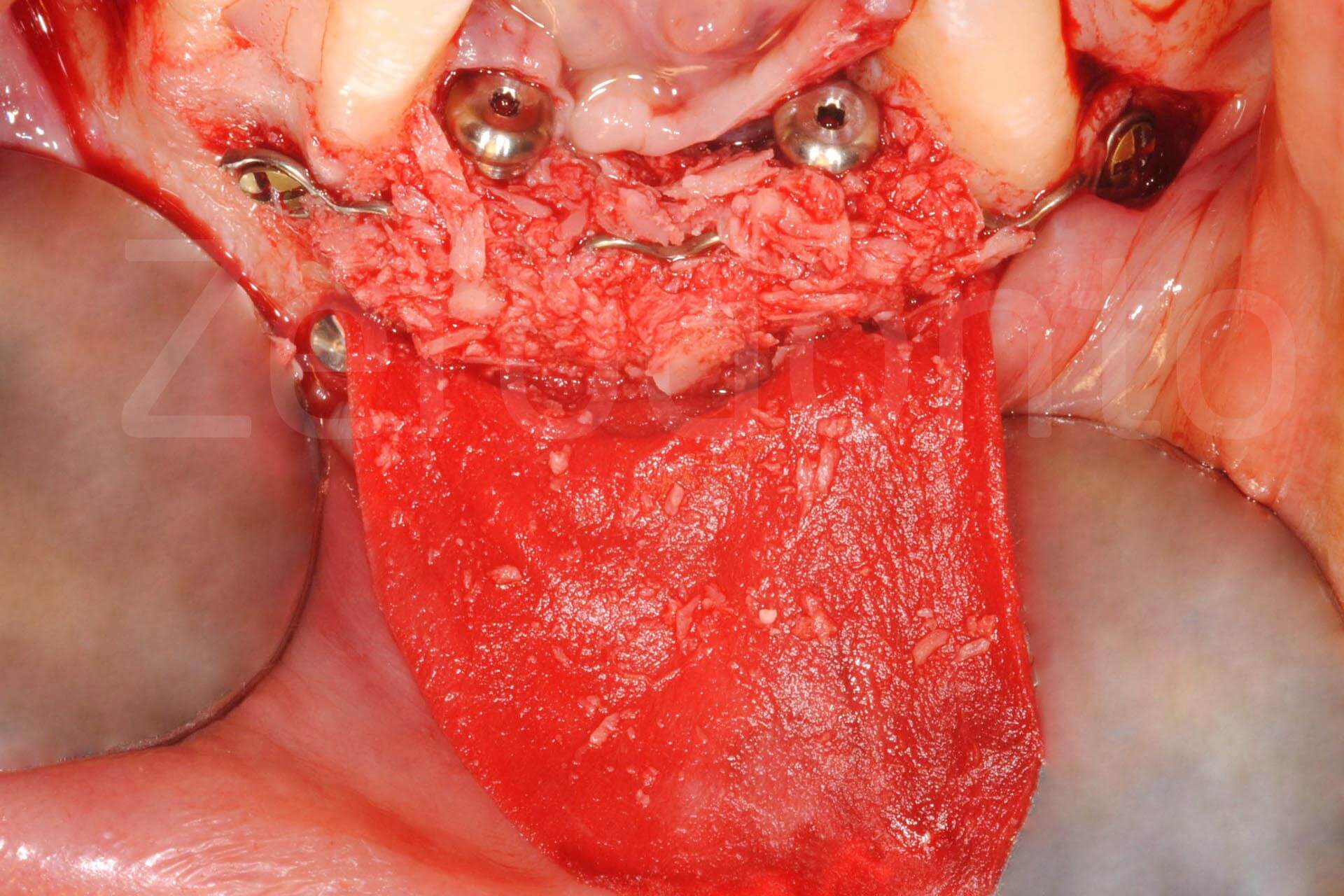
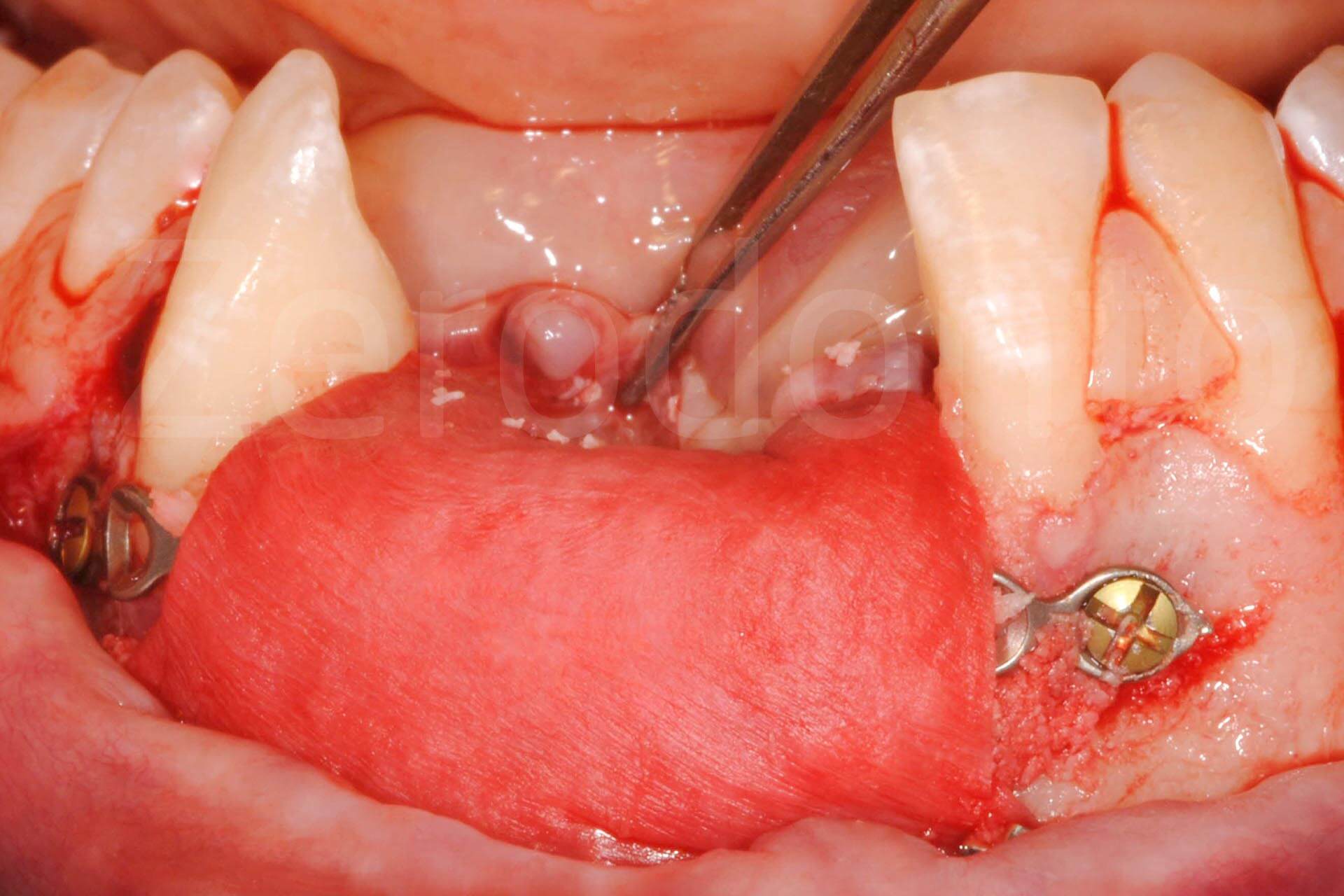
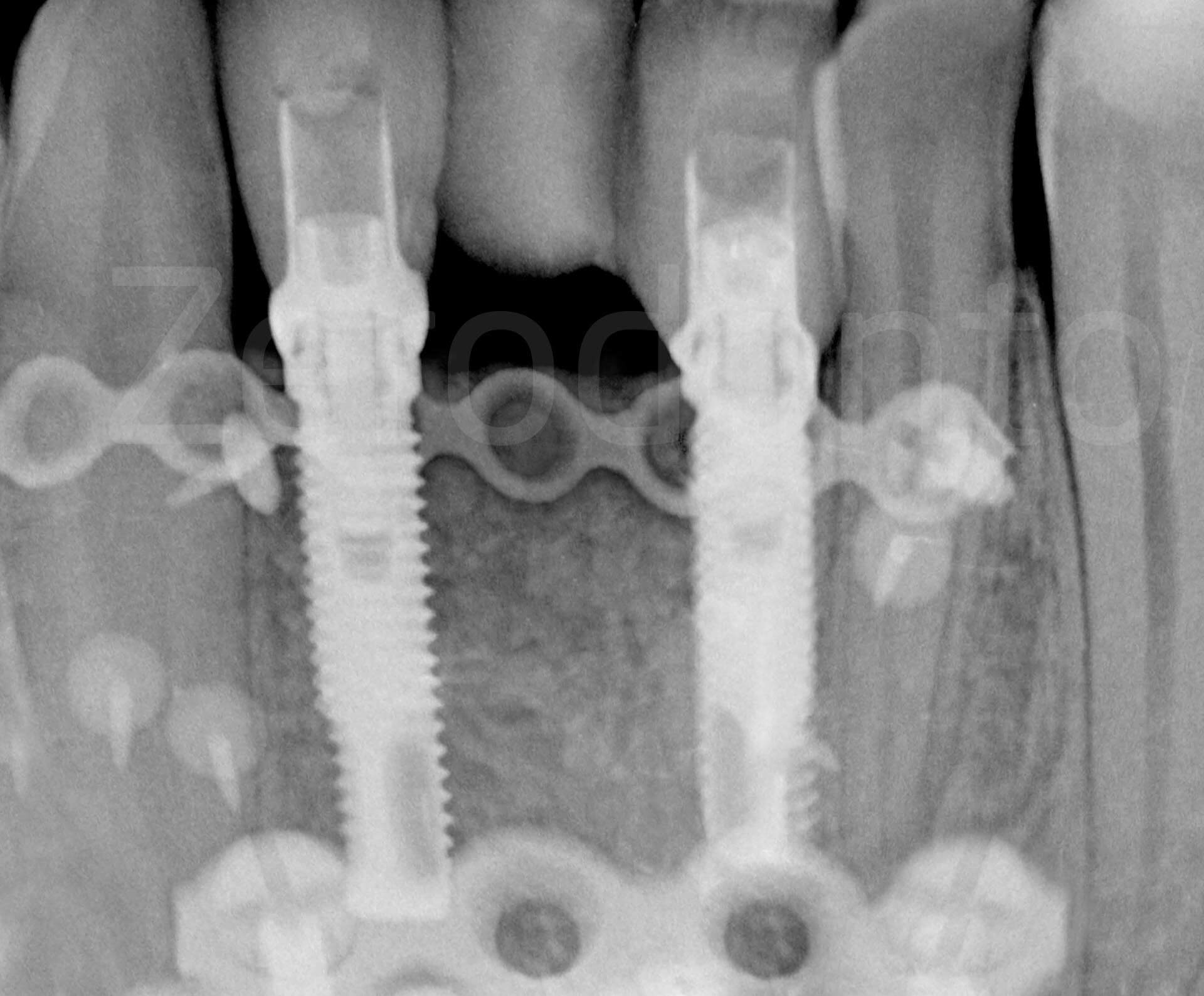
Fig. 2. Complex rehabilitation of the esthetic area: surgery
Phases of bone regeneration with prosthetically guided implant insertion.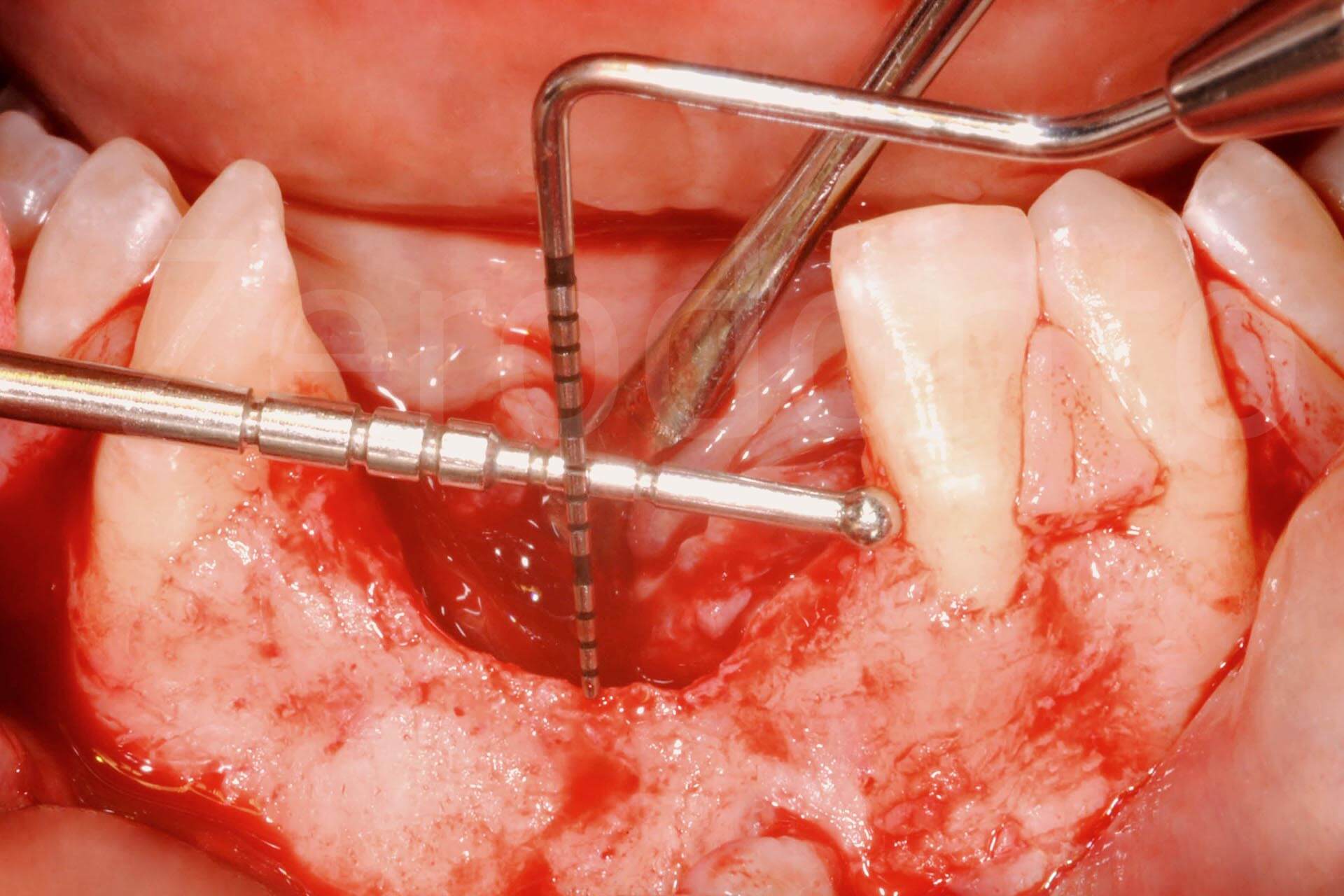
Post-surgical orthopantomography.

Tissue healing after 6 months.

Implant connection; coronal and apical epithelial-connective tissue graft increasing soft tissue thickness.
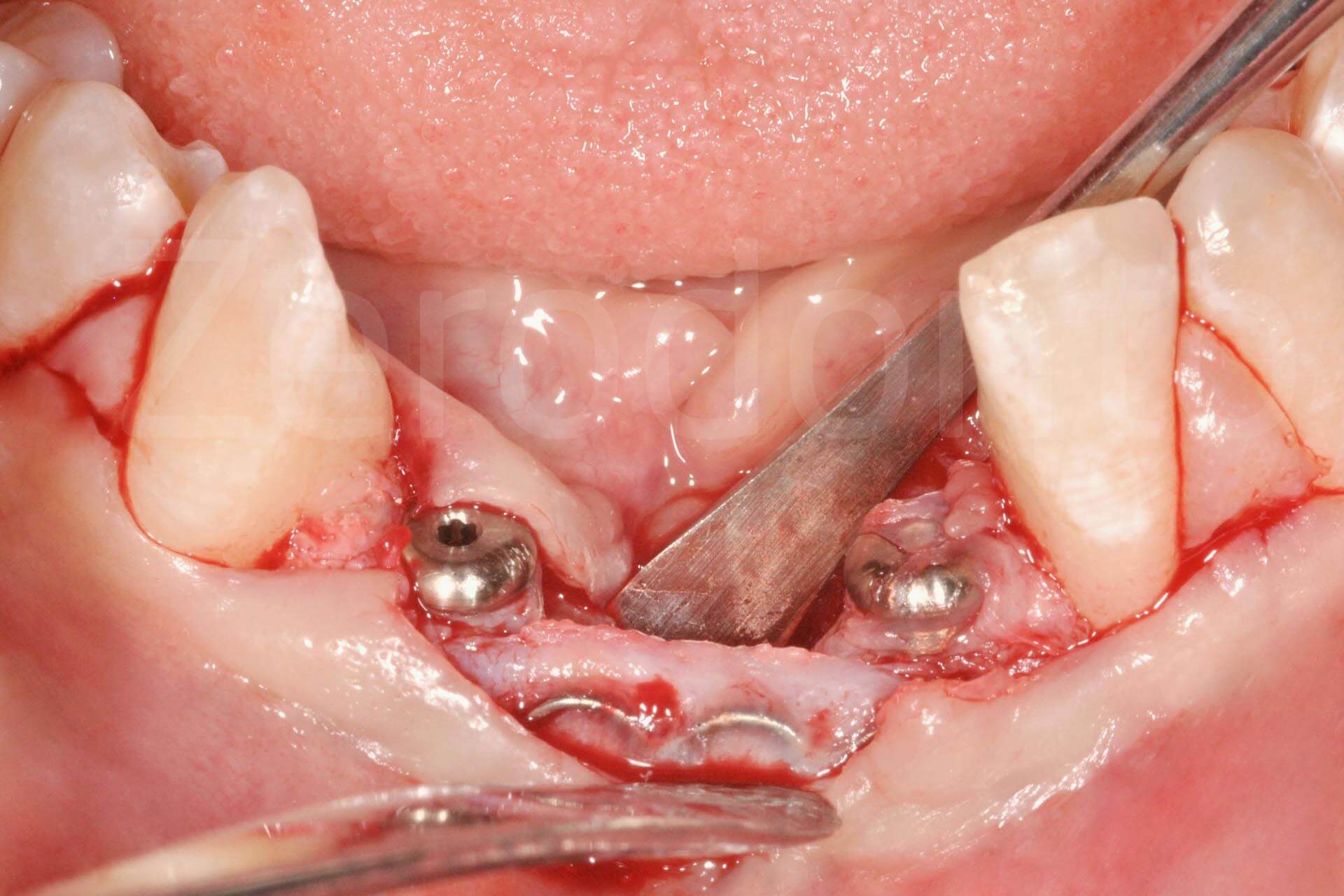
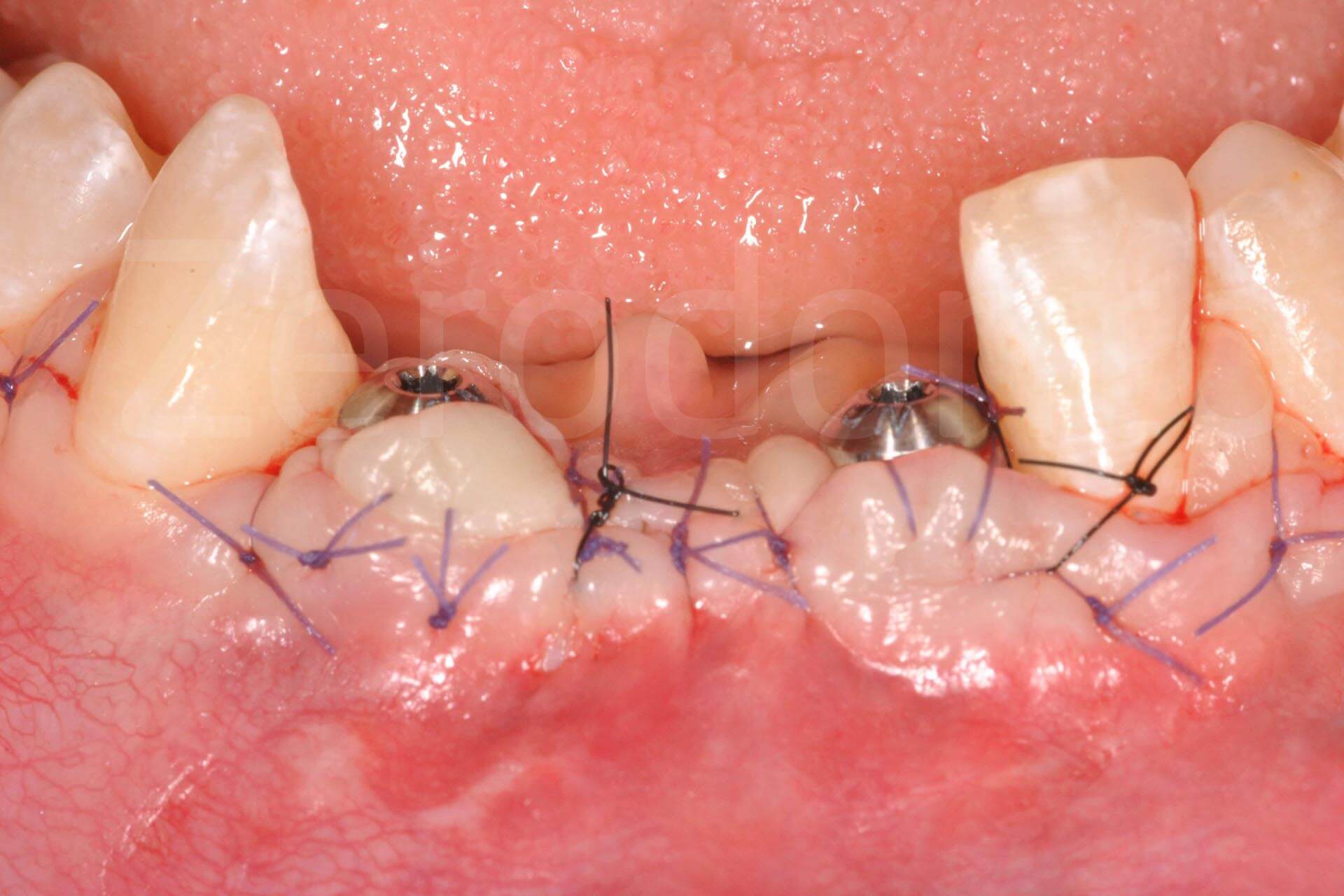
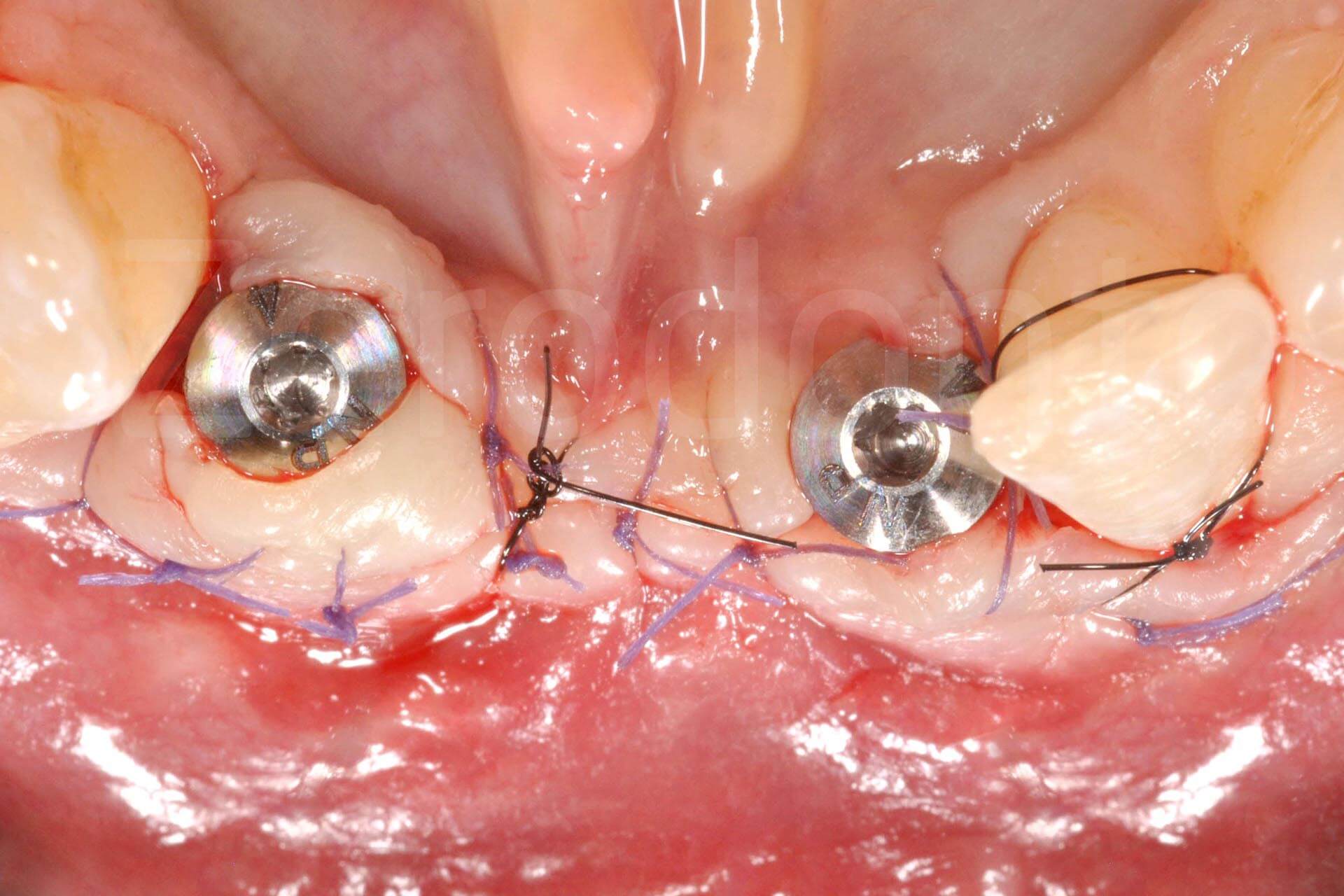
Fig. 3. Complex rehabilitation of the esthetic area: prosthetic phase
Frontal and occlusal view of provisional prosthesis.


Intraoral images of the final prosthetic rehabilitation.


Extraoral view and detail of smile at completion of the rehabilitation procedure.


Intraoral x-rays and video at 5 year follow-up.
Special features of this clinical case
Obtaining a dental implant-prosthetic rehabilitation in such a prominent vertical atrophy in the lower jaw is complex, particularly due to the difficulty in managing the soft tissue in an area where muscle traction is accentuated and where, in this specific case, scar tissue and synechiae were present as a consequence of the accident and earlier surgery.
Special observations
The vertical bone regeneration was performed simultaneously to the implant insertion, which was prosthetically guided, taking into consideration the bone peaks of the adjacent teeth. The actual bone regeneration was guided and facilitated by the position of the implants, following the Fence Technique (Merli et al, 2015), with autologous bone harvested from the symphysis, where one of the previously applied plaques was removed. Closure by primary intention was obtained through periosteoplasty (Triaca et al. 2001). A mini-invasive approach was possible by applying a collagen membrane during the second surgical phase, leaving the microplates in situ, thus reducing the extension of the flap. The soft tissue volume was increased with a bilaminar and epithelial-connective tissue graft in the coronal area.

The clinical case is an excerpt from the book “Prosthetics in Implant Therapy: The Integrated Treatment Plan” (Vol. 2, Mauro Merli, Quintessence 2016).
For further details:
Triaca A, Minoretti R, Merli M, Merz B. Periosteoplasty for soft tissue closure and augmentation in preprosthetic surgery: a surgical report. Int J Oral Maxillofac Implants 2001;16:851-856.
Merli M, Mariotti G, Moscatelli M, Motroni A, Mazzoni A, Mazzoni S, Nieri M. Fence technique for localized three-dimensional bone augmentation: a technical description and case reports. Int J Periodontics Restorative Dent 2015;35:57-64.
“Prosthetics in Implant Therapy: The Integrated Treatment Plan” (Vol. 2, Mauro Merli, Quintessence 2016).
