Dear colleagues,
below a complex case of micro-surgical endodontics by Dr. Arnaldo Castellucci.
For those who are interested, you can find the full article about the advanced techniques in micro-surgical Endodontics on our blog at the following link:
Micro-surgical Endodontics: the state of the Art
https://www.zerodonto.com/en/2010/04/micro-surgical-endodontics-the-state-of-the-art-2/

Illustrations:

Fig 1 – The previous panoramic radiographs speak by themselves. After the wrong therapy of the molar, the panoramic radiograph of 1988 shows a huge lesion involving the apexes of three mesial teeth.

Fig 2 – Then, in the panoramic radiograph of 1995 an incongruous treatment of tooth 4.5 is evident as well as a fractured endodontic instrument in the apex.
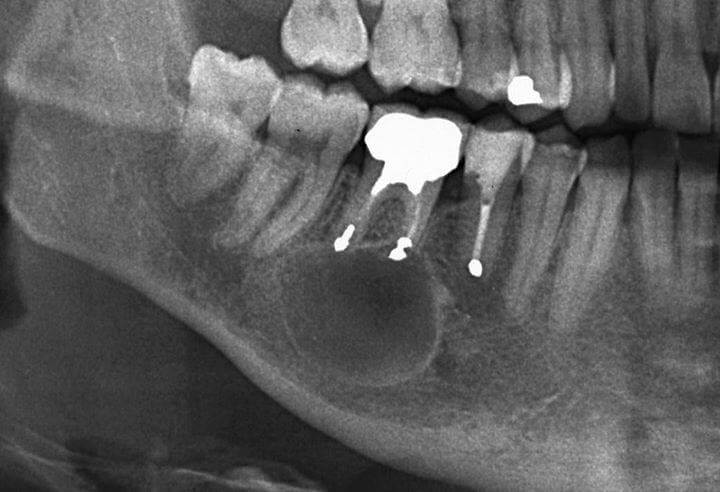
Fig 3 – Finally, the panoramic radiograph of 2011 shows the negative outcomes of an “old-fashioned” apicoectomy and retrograde obturation, performed by an oral surgeon without any magnifying system using rotary burs and amalgam.
_________
In February 2012, the patient had been addressed to a maxillo-facial surgeon in order to extract the molar and remove the cyst; however, another patient, who had received a little time earlier an apicoectomy and retrograde obturation by myself, referred the patient to my office.
After checking the periodontal health around the molar so as to exclude any root fracture and after verifying the possibility to retract the cheek for a proper surgical access, I established the appointment to treat the patient.
During the surgical procedure performed through a paramarginal incision, I removed from the lesion a huge amount of pus as thick as I’ve never seen before and I enucleated the entire cyst with no difficulty.
Then, I removed the previous amalgam obturations, prepared the correct retrograde cavities including the isthmuses and sealed them using white MTA. In order to fill the residual cyst cavity, I used the most easy-handling and cheapest material: the patient’s blood. (Fig.4-6)
The sutures were removed 48 hours after surgery and today no scar is present.
The symptoms the patient complained completely disappeared soon after the treatment and nowadays the patient can chew using his own tooth, with no extraction or implant.
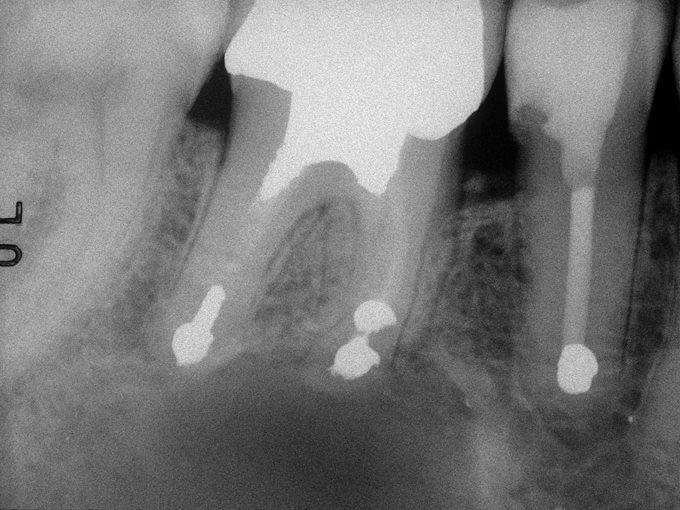
Fig 4 – Pre-op x-ray before the micro-surgical retreatment. The old amalgam obturations were removed, correct retrograde cavities including the isthmuses were prepared.

Fig 5 – Post-op x-ray after the micro-surgical retreatment. The canals were sealed using white MTA. In order to fill the residual cyst cavity, the most easy-handling and cheapest material was used: the patient’s blood.

Fig 6 – 9 months post-op x-ray.
_________
I would kindly remember to anybody that up to date Surgical Endodontics (and not Endodontic Surgery, which is completely different…) shows success rates very close to 100% in the long-term, if it is performed correctly, with proper knowledge, with proper handling, magnification (microscope) and materials (MTA)!!! Moreover, I’d like to remember to Sirs oral implant surgeons that oral implants are useful to replace missing teeth but not to substitute existing teeth, that the best “implant” is a natural tooth and, finally, that in Dentistry as well we should follow the teachings of the New Testament: “Do unto others as you would have them do unto you”. So, before taking the dental forceps, think about the best treatment you would like for yourself…
See photogallery on Facebook.
