The need to work under dry conditions, free of saliva, has been recognized for centuries, and the idea of using a sheet of rubber to isolate the tooth dates exactly 153 years! The introduction of this notion is attributed to a young American dentist from New York, Sanford Christie Barnum, who in 1864 demonstrated for the first time the advantages of isolating the tooth with a rubber sheet.
Dr. Christie S. Barnum.
“At that time when the idea of rubber dam dawned on my mind, I was practising in Monticallis, Sullivan Co., New York. It was the result of much persecution from the inroads of saliva. I had spent many an hour, weary and distracted, battling against its incursions. Many a sleepless night had I over sad failures… with the one absorbing question ever before me unanswered. “How shall I keep the cavities dry?” The answer came… on the 15th day of March 1864, a case presented itself of a cavity in a lower molar standing alone, on the left side, in a mouth, as wet – well as water gushing from every duct could make it. In a sort of half desperate way, and partly to try the new idea, I cut a hole in my napking protector and over the tooth it went. There was the rubber dam”.1
At that time, keeping the rubber in place around the tooth was problematic, but things soon improved a few years later, when in 1882 S. S. White introduced a rubber dam punch similar to that used still now.
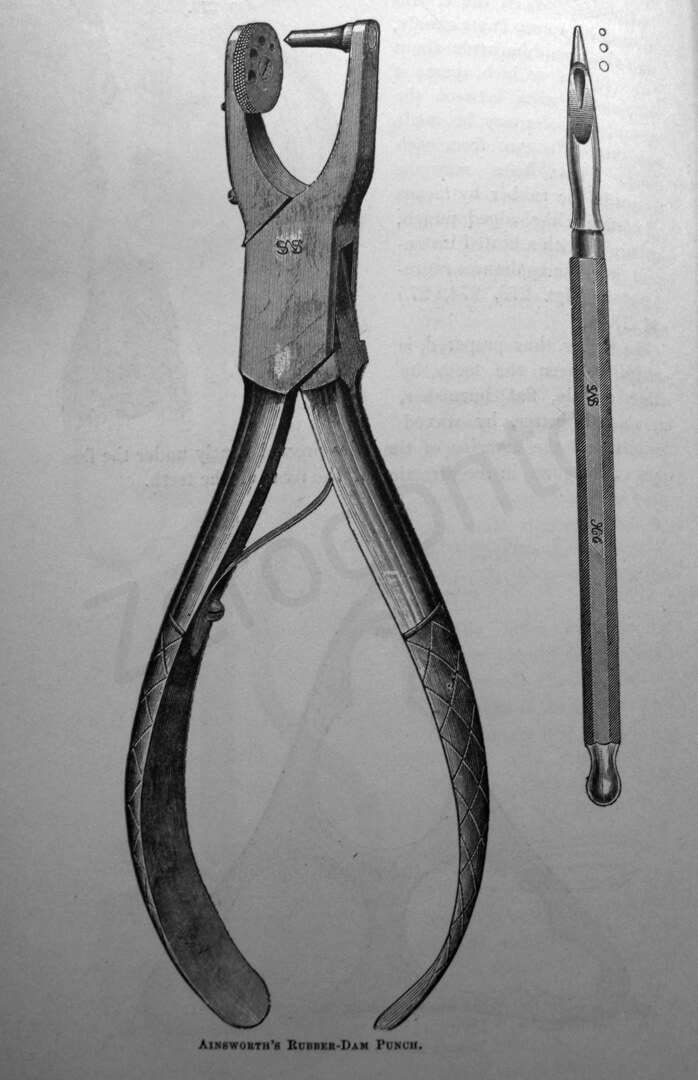
Rubber dam punch introduced by S. S. White in 1882.
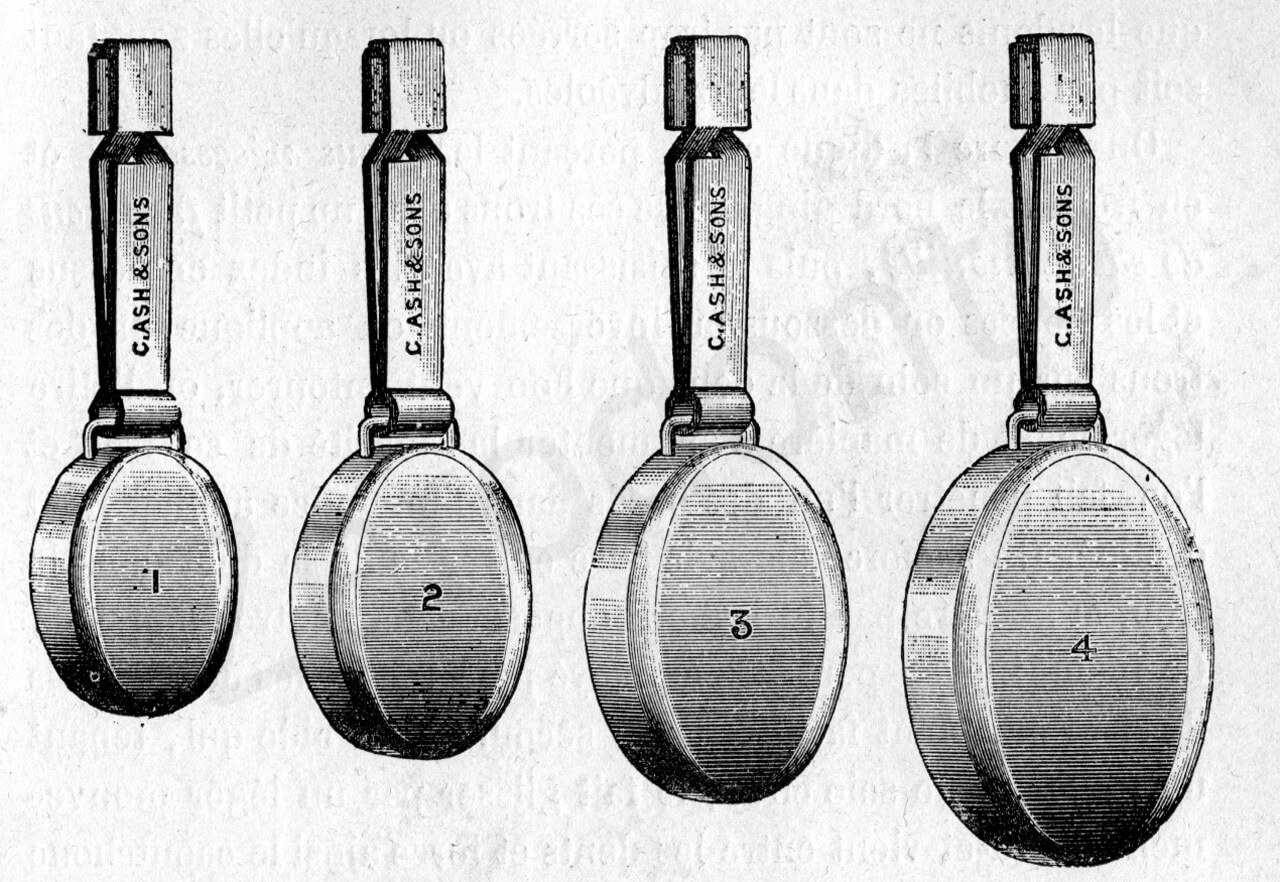
In the same year Dr. Delous Palmer, and later Dr. Stokes and Dr. Elliot, introduced a set of metal clamps which could be used for different teeth.2
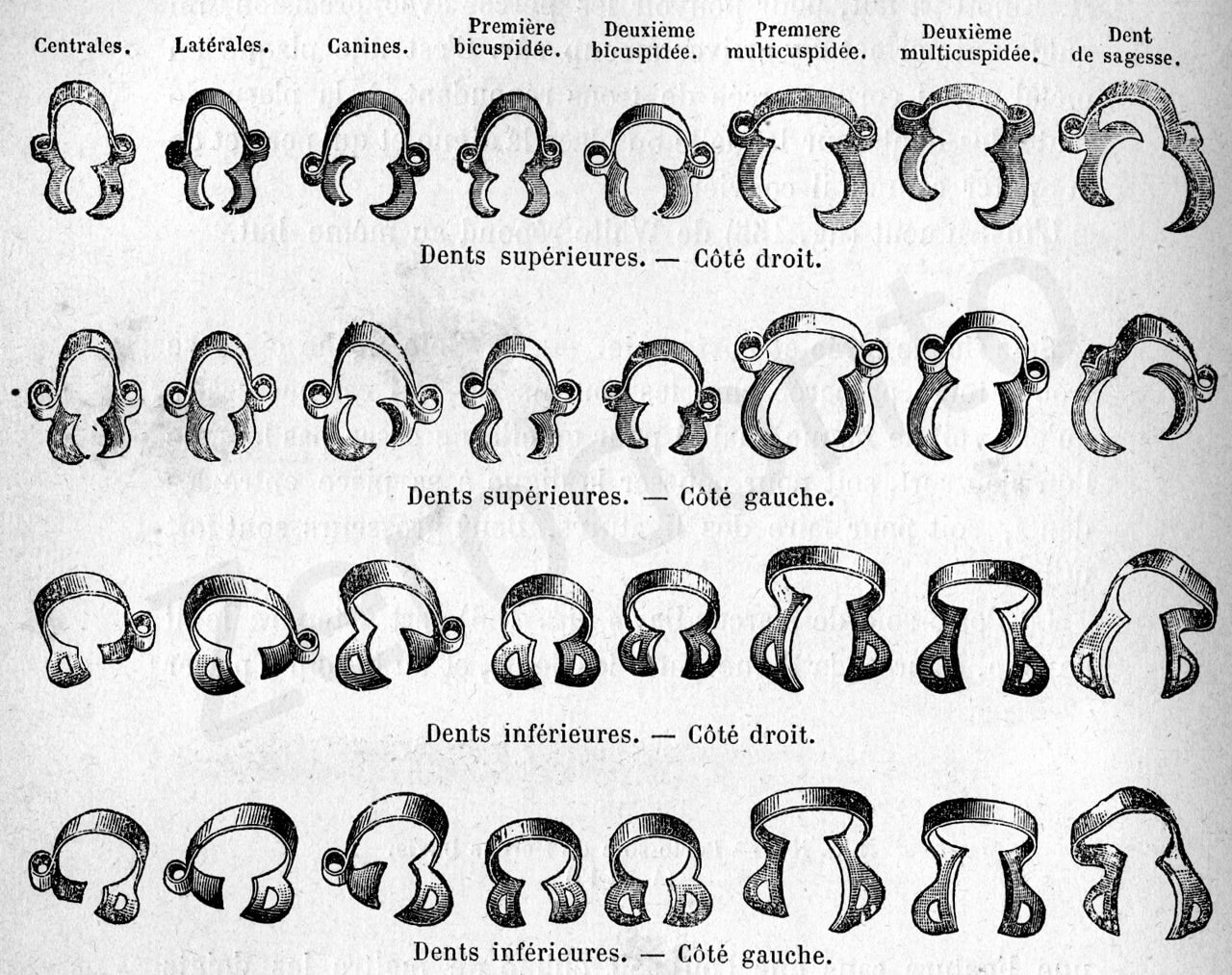
Set of metal clamps introduced by Dr. Delous Palmer in 1882
Metal clamps designed by Dr. Stokes

Metal clamps designed by Dr. Elliott. (From: Andrieu E.: Traité de Dentisterie Opératoire, Octave Doin Ed., Paris 1889).
This said, it seems incredible that even today, two centuries later and living now in the third millennium, there are still dentists who are not convinced of the usefulness of this very simple rubber sheet.
The American Associations of Endodontists in its Quality Assurance Guidelines and Position Statement of 2010 says that “Tooth isolation using the dental dam is the standard of care; it is integral and essential for any nonsurgical endodontic treatment. One of the primary objectives of endodontic treatment is disinfection of the root canal system. Only dental dam isolation minimizes the risk of contamination of the root canal system by indigenous oral bacteria. The dental dam also offers other benefits, such as aiding in visualization by providing a clean operating field and preventing ingestion or aspiration of dental materials, irrigants and instruments.”3
The European Society of Endodontiology in the Quality Guidelines says that “Root canal treatment procedures should be carried out only when the tooth is isolated by rubber dam to: prevent salivary and bacterial contamination, prevent inhalation and ingestion of instruments and prevent irrigating solutions escaping into the oral cavity.4
According to the author’s opinion, when it is not possible to isolate the tooth with the rubber dam, the clinician has two options: one is to make it possible and the other is to extract the tooth! There is no other choice.
The operative procedures that are performed in the patient’s mouth must be seen as larger or smaller surgical procedures. In dentistry, as in general surgery, isolation of the operative field is imperative, even for a simple filling.
Even more so than in restorative dentistry, the rubber dam is obligatory in Endodontics,5 so much so that Endodontics should not be performed without a dam. Furthermore, an endodontic treatment should not be undertaken unless the tooth – particularly if damaged – has not been reconstructed to allow easy positioning of the rubber dam. There should be no excuse for not using the rubber dam in Endodontics; the law should severely punish the dentist who causes serious injury, including death, to a patient because he/she did not use one.6-23
Patick Wahl in a recent article says that in the United States any law suit is lost if the rubber dam has not been used.24
The only tooth that may be treated without the rubber dam is the tooth that is so severely damaged that the only instrument to be used are the extracting forceps. As Aiello 25 states, one must recall that the rubber dam clamp occupies the future position of the marginal closure of the prosthetic crown. It is therefore unthinkable to endodontically treat a tooth on which the rubber dam cannot be assembled, since it is not known whether and how the tooth will be restored.
A contraindication to the use of the rubber dam is a patient’s allergy to the chemical constituents of rubber.26,27 In this circumstance, albeit rare, the teeth may be isolated with polythene sheets,28 which impose limitations related to the lack of elasticity of this material as compared to rubber. Today “no-latex” dam is available,29 to be used on allergic patients. This new dam has the same elasticity and it is even more resistant to corrosion when in contact with endodontic solutions like sodium hypochlorite or endodontic solvents like chloroform.
No-latex rubber dam, for allergic patients.
There are odd rumors about the use of the rubber dam; for example, it is claimed that it takes too much time to assemble. Cragg 30 correctly states that “that which takes more time, with respect to the rubber dam, is trying to convince the dentist to use it.”
It is worth spending a few seconds to assemble the rubber dam for use in endodontic procedures and thus improve the entire treatment.
In Endodontics, use of the rubber dam confers the following advantages:
- The patients are protected from the ingestion 10 (Fig. 5) or, worse, the aspiration 7 (Fig. 6) of small instruments, dental fragments, irrigating solutions, or irritant substances.
- The opportunity to operate in a clean surgical field.
- Retraction (very important for working in the posterior areas) and protection of the soft tissues (gums, tongue, lips, and cheeks) (Fig. 7), which are sheltered from the cutting action of the bur.
- Better visibility in the working area. The advertisement of a famous manufacturer of instruments for the assembly of the rubber dam correctly reads: “Do better what you see and see better what you do.”
- Reduction of delays: the patients, with fortunately rare exceptions, cannot converse except with great difficulty; besides, they will not have to rinse their mouth every five minutes.
- The dentist and dental assistant are protected against infections which can be transmitted by the patient’s saliva.17
- The dentist is more comfortable, as he/she may work at a more leisurely pace and may be permitted to answer an important telephone call, leaving the patient well protected with the rubber dam and the dental assistant close to him/her.
- Better tactile sensitivity during the cleaning and shaping procedure. Without the rubber dam, the dentist, aware of the risk of causing the patient to ingest or aspirate an instrument, holds the files in such as way that they will not slip from his/her fingers. The pressure applied to the handle of these instruments reduces the sensitivity of the fingers and precludes the use of the instruments to perform delicate procedures. With the rubber dam in place, on the other hand, the instruments may be held delicately, without fearing that they may slip from operator’s hand.31
- The patients are more comfortable, as they do not feel that their mouth is invaded by hands, instruments, and liquids.

Fig. 5. This radiograph shows the presence of an endodontic instrument among the intestinal loops. Few weeks later, the patient died!44

Fig. 6. This radiograph shows the presence of an endodontic instrument lodged in the upper respiratory tract. This patient died!

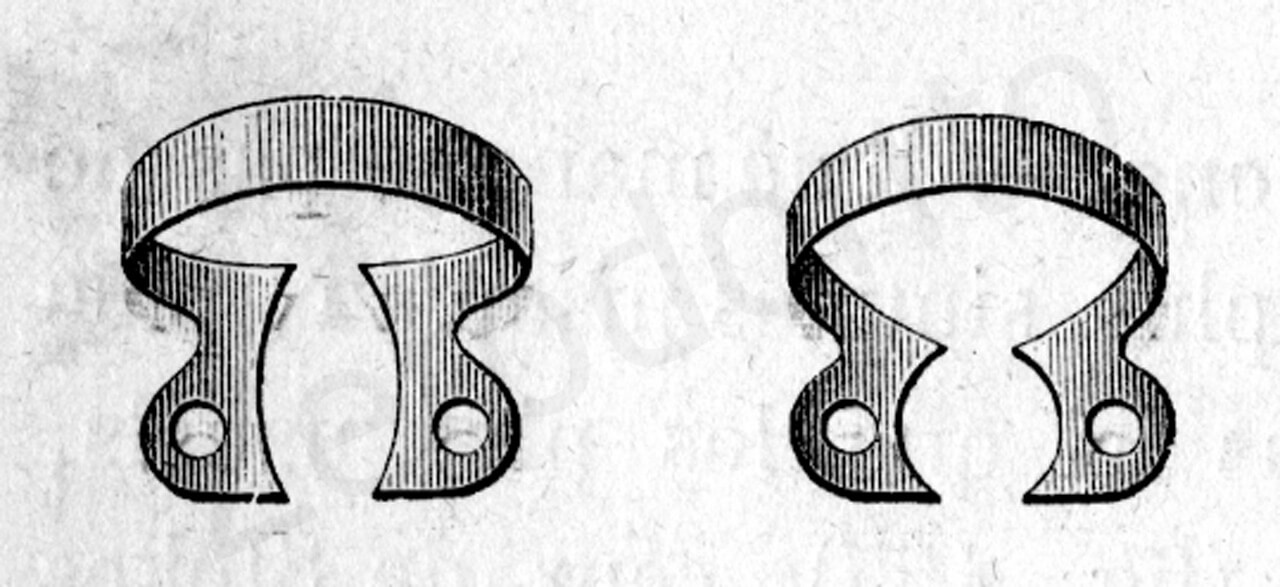
Fig. 7. To improve protection of soft tissues, some of the old clamps designed by Palmer were made with tongue-guards. (From: Harris C.H.: Principles and Practice of Dentistry, Gorgas F.J. ed., P. Blakiston, Son & Co., Philadelphia 1885).
Patients increasingly appreciate the use of the rubber dam. On occasion, they may ask whether it is a new invention,32 and once they have tried it, they do not want to do without it in the future.
INSTRUMENTS
To facilitate the assembly of the rubber dam, it is advisable to have the appropriate instruments within arm’s reach. This is simpler than it might appear.
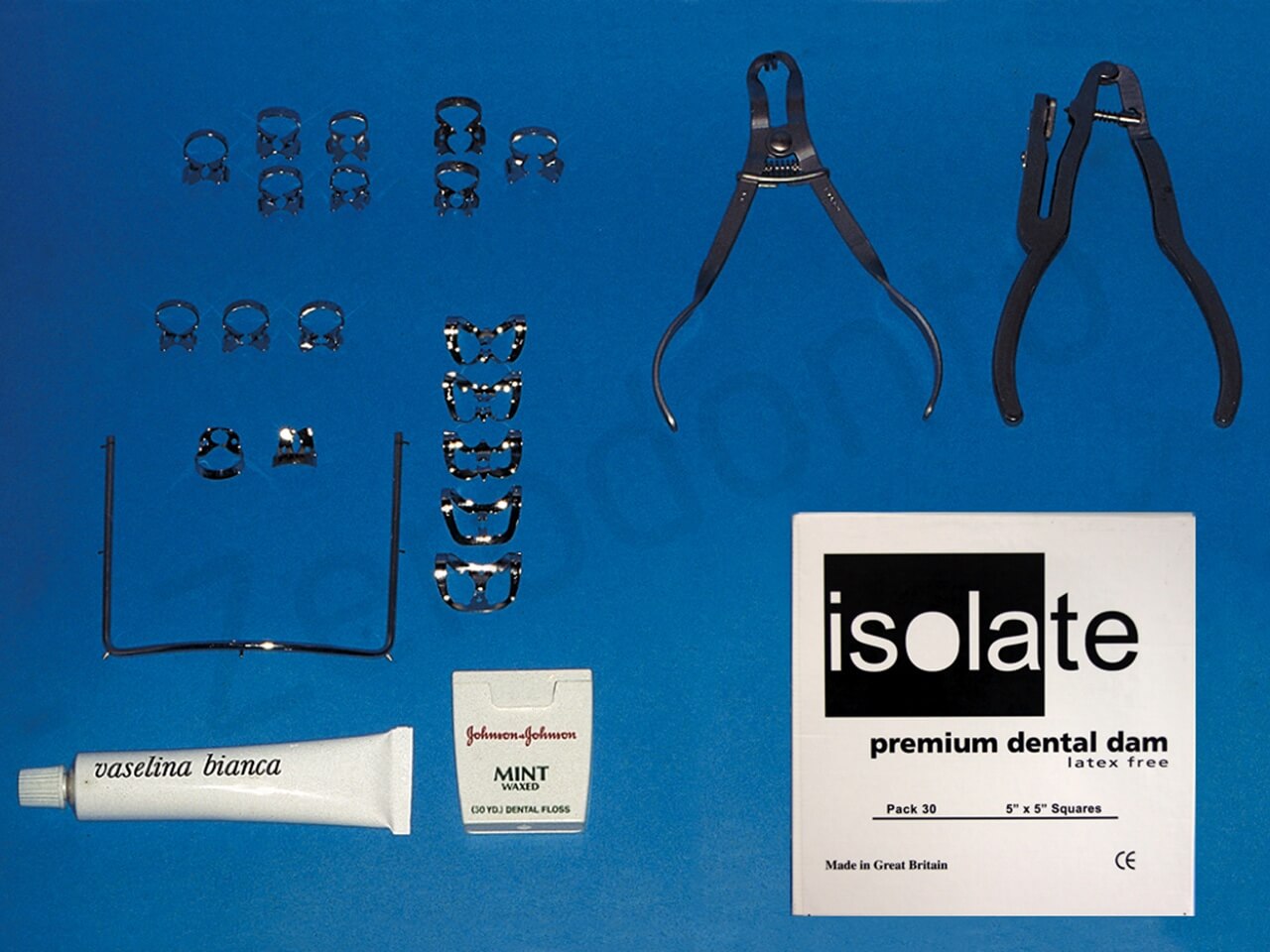
Minimum set of instruments necessary for the assembly of the rubber dam in the different sectors of the mouth.
1) Rubber Dam
The dam comes in different sizes (5″ x 5″ inches and 6″ x 6″ inches, as well as rolls), colors (light, blue, gray, and green), and thicknesses (special heavy, extra heavy, heavy, medium, and thin).
The 6″ x 6″ format is useful in restorative dentistry, where it is necessary to isolate several teeth at the same time. In Endodontics, where one tooth is isolated at a time, the 5″ x 5″ format is more than sufficient, even for working in the posterior sectors of the mouth.
Some prefer the dark colors, since the tooth stands out better, but it is really a question of habit. The light-colored dam is slightly transparent, unlike the other colors, which may be helpful in positioning the intraoperative radiograph.
The quality of the dam sheets deteriorates with time; in particular, they lose elasticity. One should therefore stock them in moderate quantities, keep them refrigerated, observe the expiration date on the back of the box, and obtain one’s supplies from a distributor that sells them at high volume, so as to avoid buying supplies that have already been in the warehouse for a long period of time and have thus already expired.
To test them, one can perform the same test as that to check the adequacy of the dam punch: just after punching a hole in the dam, it is stretched in different directions to confirm that it does not tear.
2) Rubber Dam Punches
It is used to make round holes of different diameters (0,7 – 2 mm), depending on the tooth to be isolated. Several brands are available. Nonetheless, it is necessary to check whether the dam opening is exactly round, without irregularities. To determine this, it suffices to punch a hole in a dam sheet and then enlarge this opening by stretching the sheet in different directions. The dam should not tear.
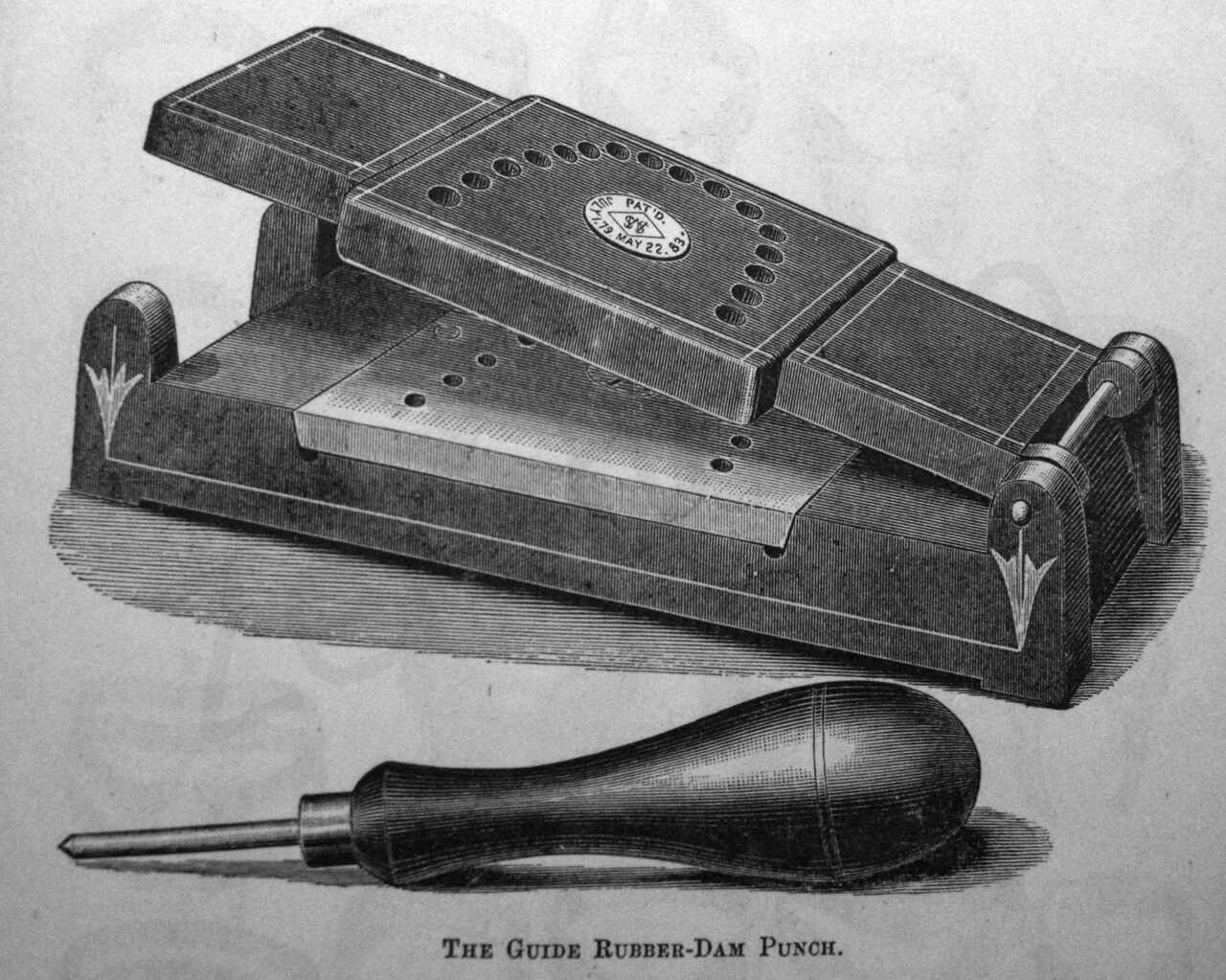
The old S.S. White rubber dam punch of the XIX century.

A modern rubber dam punch.
3) Rubber dam clamps
The fit of the rubber dam essentially depends on the choice of the appropriate clamp and its correct positioning.
The clamps are classified as winged or wingless. The dentist may choose those with which he feels more comfortable.

Clamps for the front teeth.

Clamps for the premolars

Clamps for the molars. Winged.

Clamps for the molars. Wingless.
The positioning techniques vary slightly, but the final result is the same. Sometimes wingless clamps are preferable, inasmuch as they are less bulky and may be used easily in the posterior sectors in patients with particularly thick cheeks.
The most commonly used are:
FRONT TEETH:
IVORY # 6
IVORY # 9
IVORY # 90N
IVORY # 212S
IVORY # 15
PREMOLARS:
IVORY # 1
IVORY # 2
IVORY # 2A
MOLARS THAT ARE COMPLETELY ERUPTED, WHOLE, OR COVERED BY FULL CROWNS:
IVORY # 7
MOLARS THAT ARE INCOMPLETELY ERUPTED OR ALREADY PREPARED FOR A FULL CROWN:
IVORY # 14
IVORY # 14A
IVORY # 7A
ASYMMETRICAL MOLARS, IN PARTICULAR THE SECOND AND THIRD:
IVORY # 10
IVORY # 11
IVORY # 12A
IVORY # 13A
WINGLESS, TO BE USED WHEN THE WINGS OBSTRUCT THE WORKING FIELD:
IVORY # W8A
IVORY # 26N
The clamps may also be modified to improve their grip and allow a more precise fit.33 Moreover, there is no reason not to use a premolar clamp on a small molar or frontal tooth, or a # 9 clamp on a hemisected root of a lower molar; any such adaptation is permitted, as long as the final result – correct placement of the rubber dam – is achieved.
The only danger is fracture of the rubber dam clamp once it has been positioned in the mouth. If this occurs, the elasticity of the dam will cause the fragments to be ejected from the patient’s mouth. It is therefore prudent to secure the clamp with dental floss and anchor it to the dam frame.
4) Rubber Dam Clamp Forceps
This instrument is necessary to open the clamp and position it around the tooth.
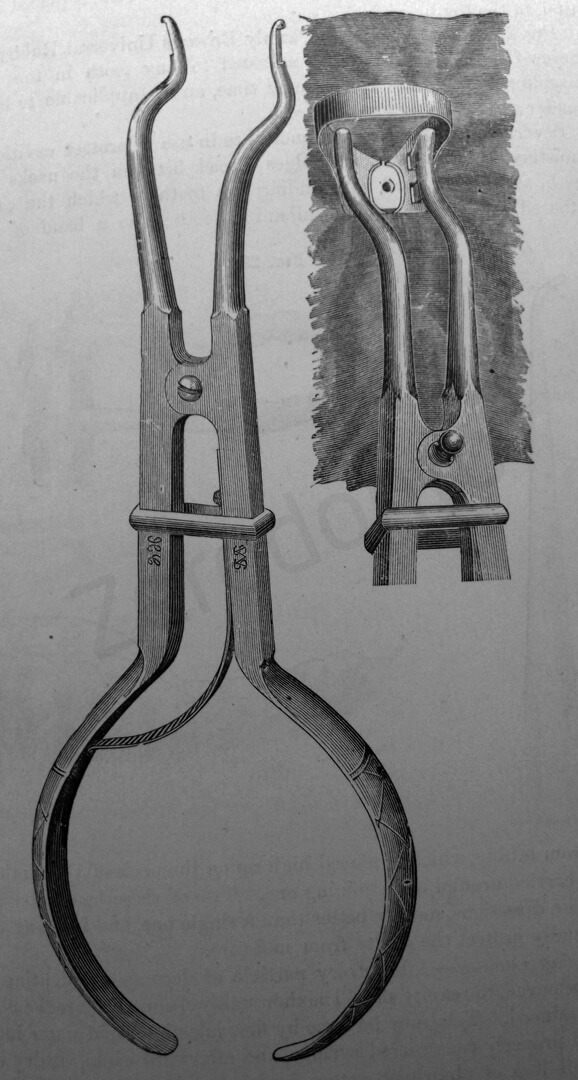
An old rubber dam clamp forcep
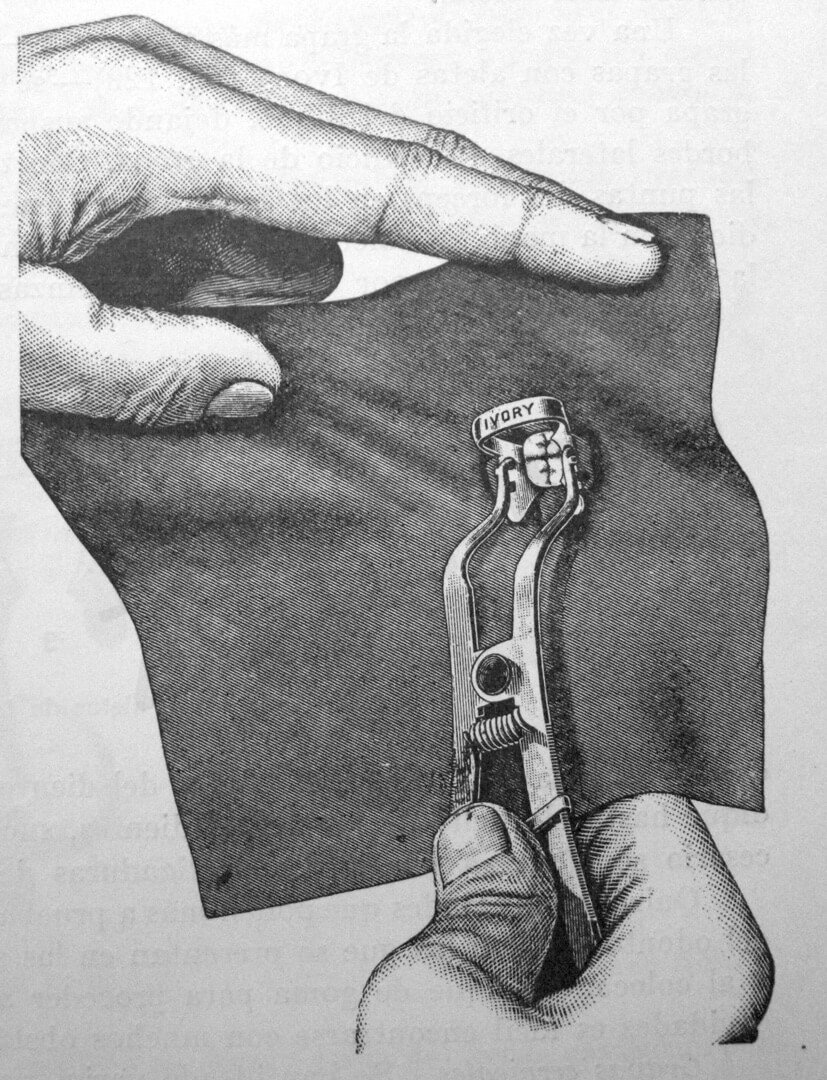
The Ivory forceps are preferable, because they allow the dentist to apply direct pressure toward the gum, which is frequently necessary to position the clamp securely below the bulge of the tooth crown.

The new Ivory clamp forcep
5) Rubber Dam Frame
This is necessary to maintain tension in the dam so that the lips and cheeks may be retracted well. Some frames, including the Young frame, are made of very thin metal; others, including the Nygaard-Ostby or Starlite frame, are plastic. In comparison to the Young frame, the latter have the advantage of being radio-transparent; on the other hand, they are bulkier.
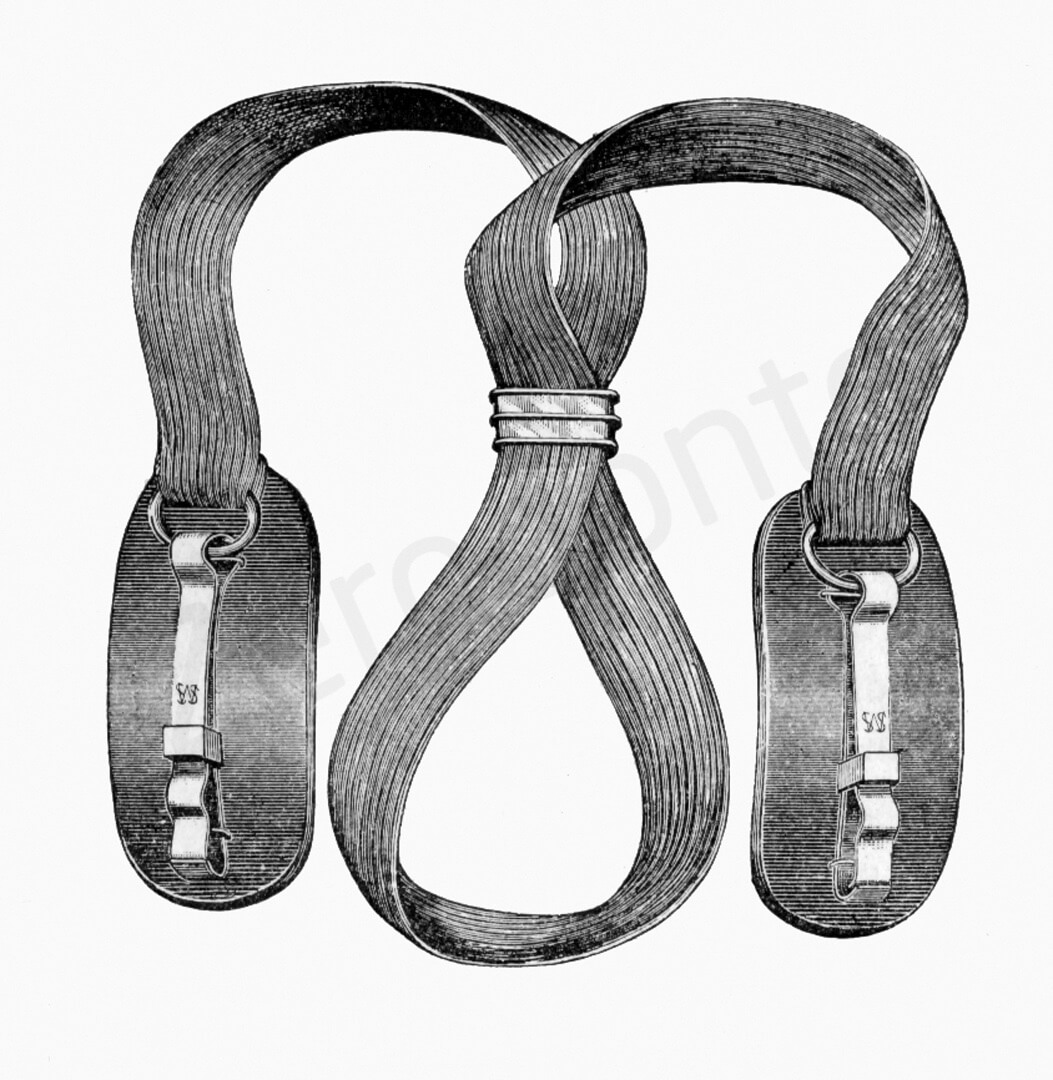
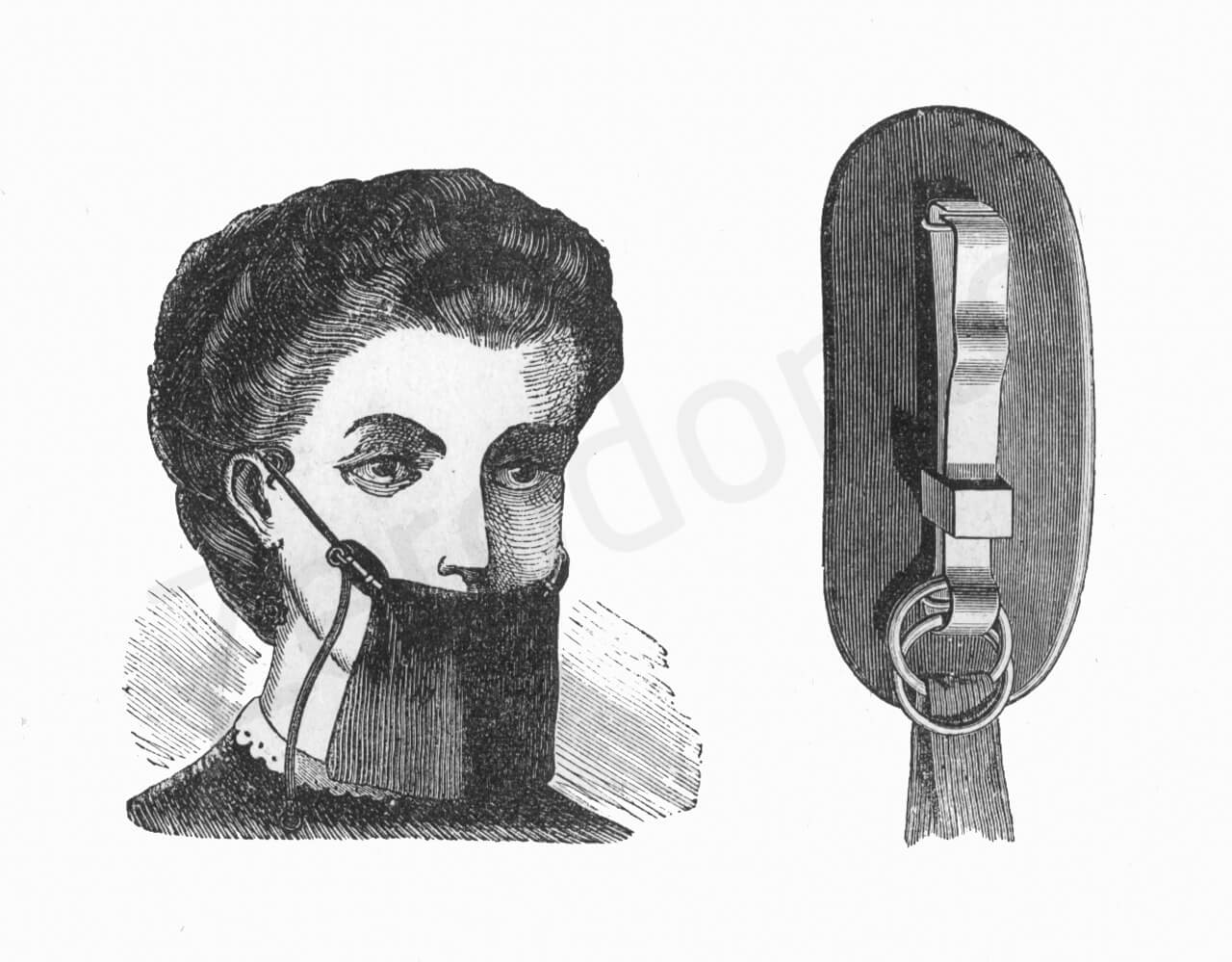
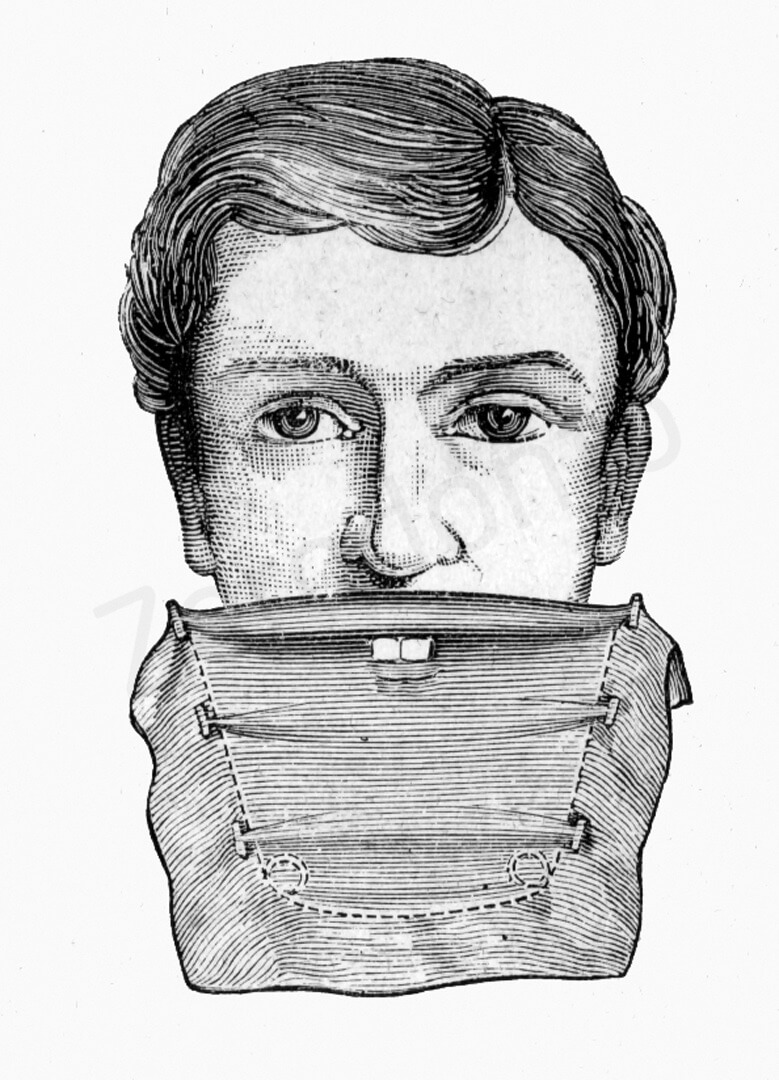
Dam tensors such as those of Woodburg,34 Cogswell, Mitchell, and Fernald,2 which are based on the principle of maintaining tension in the dam by the use of clips and elastic bands passing directly over the nape of the neck, are out-dated and have no use in modern Endodontics.
Woodburg’s rubber-dam tensors, which are no longer used
Mitchells’ dam holders
Dr. Cogswell’s dam holder
Dr. Cogswell’s dam holder
Dr. Fernald’s dam holders

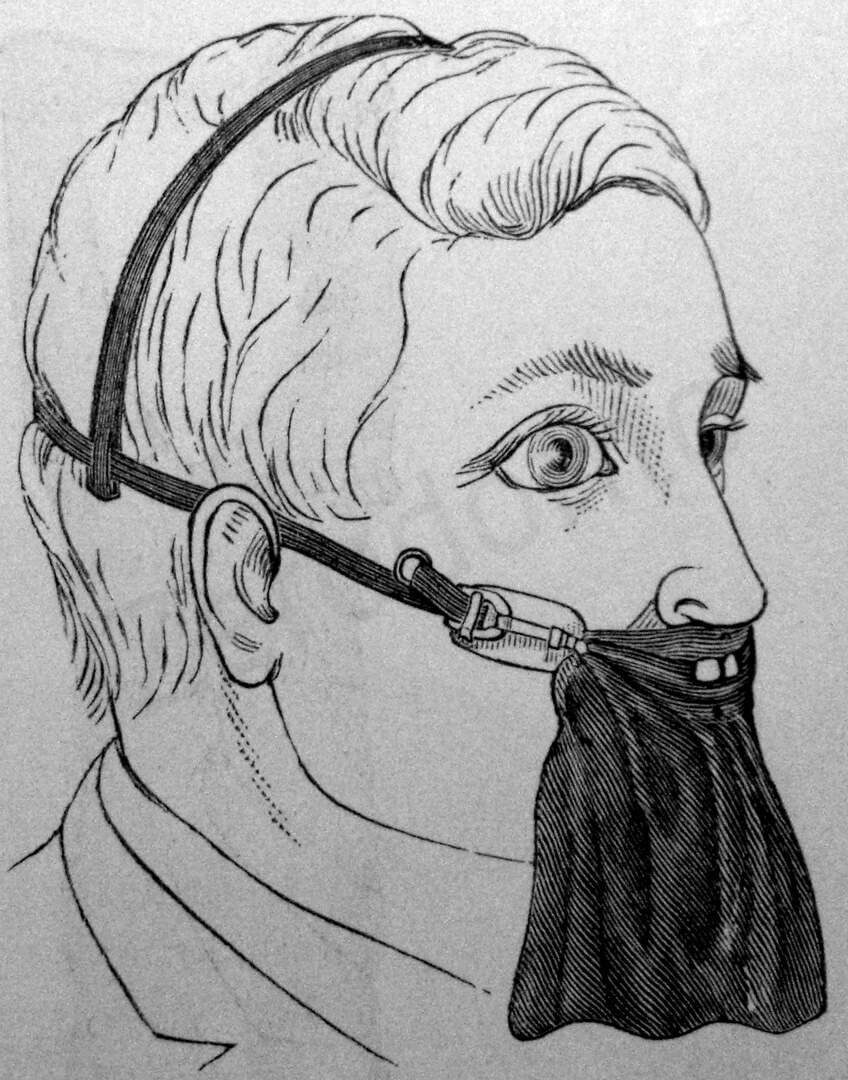
The Brasseur’s rubber dam in place. (From: Andrieu E.: Traité de Dentisterie Opératoire, Octave Doin Ed., Paris 1889).
Furthermore, they have numerous disadvantages: they require more time for positioning; they completely cover the patient’s nose and mouth, giving him the unpleasant sensation of suffocation; and they do not cause the least bit of retraction of the lips or cheeks, like the others.
New rubber dams recently introduced in the market are the Handidam (Aseptico, Woodinville, WA) and the Insti-Dam (Zirc Company, Buffalo, MN), two rubber dam systems with built-in foldable radiolucent plastic frame.

The Insti-Dam (left) and the Handidam (right).
6) Lubricant
Before positioning the dam, it is advisable to lubricate the inner surfaces well with Vaseline or, more simply, tooth paste, so that the sheet will slide better over the contours of the teeth, more easily overcome the contact areas mesially and distally, and close tightly around the cervix of the tooth.
7) Rubber Dam Napkins
These prevent direct contact between the rubber sheet and the patient’s cheek. By absorbing the saliva that accumulates beneath the dam by capillary action, they facilitate treatment. Their use is not mandatory; however, they are particularly indicated in cases of allergy to the rubber of the dam.
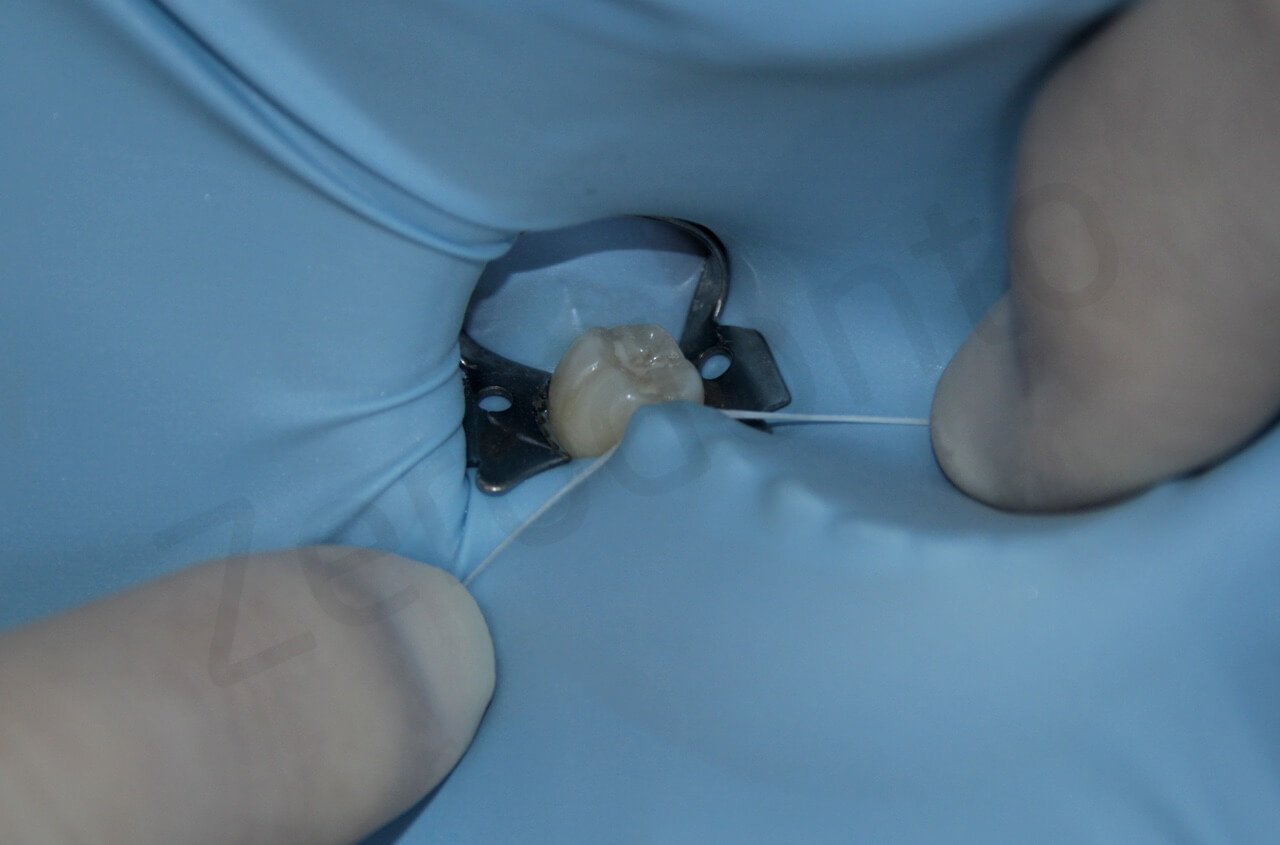
8) Dental Floss
Apart from preventing the ingestion or aspiration of the clamp, dental floss is particularly useful for assessing the condition of the mesial and distal contact areas, and thus for facilitating the passage of the rubber sheet beneath them.
9) Assistant
The dentist may position the rubber dam on any tooth using only his hands, but it is obvious that this procedure is facilitated by the help of an assistant.
The rubber dam can be placed without the help of the dental assistant. (From: Harris C.H.: Principles and Practice of Dentistry, Gorgas F.J. ed., P. Blakiston, Son & Co., Philadelphia 1885).
POSITIONING OF THE DAM
After using dental floss to check the nature of the contacts

The use of dental floss provides information about the contact areas
and determine whether there is welding between prosthetic crowns or whether there are irregularities of old restorations that need to be eliminated, one selects the clamp that one thinks might be appropriate for the case and tries it in the mouth.

The clamp is positioned around the tooth in such a way that it is stable and does not damage the periodontal tissues. Dental floss has been tied to this clamp for security reasons. If it slipped off during the trial placement, it could be swallowed or aspirated. If it broke while being opened with the rubber dam clamp forceps, the lingual part could easily disappear into the patient’s throat.

Same precaution for a front tooth
It is advisable to secure the clamp with dental floss, to protect the patient from the ingestion or the aspiration of the clamp. If it comes off easily, it should be changed. If it appears stable, one inserts it in the opening of the rubber sheet, which should already have been prepared.

The rubber sheet is punched with the rubber dam punch
The rubber dam is stretched over the wings of the selected clamp

The rubber dam is stretched over the wings of the selected clamp

With the help of an assistant, the dam and clamp are placed in position in the patient’s mouth

The rubber dam clamp forceps positions the clamp around the tooth to be treated

Young’s frame is positioned to produce tension in the dam

Young’s frame is positioned to produce tension in the dam

Using an instrument, the dam is slipped beneath the clamp wings

Using an instrument, the dam is slipped beneath the clamp wings
Dental floss is used to force the dam through the interproximal contacts

Dental floss is used to force the dam through the interproximal contacts
Initially, it may be difficult to position the opening correctly so that the dam disturbs neither the dentist nor the patient. The posterior teeth may present greater problems. In these cases, it is advisable to punch the opening more centrally than suggested by the commercially available stamps or at the point corresponding to the imaginary ellipse that represents the distribution of the teeth in the patient’s two arches.
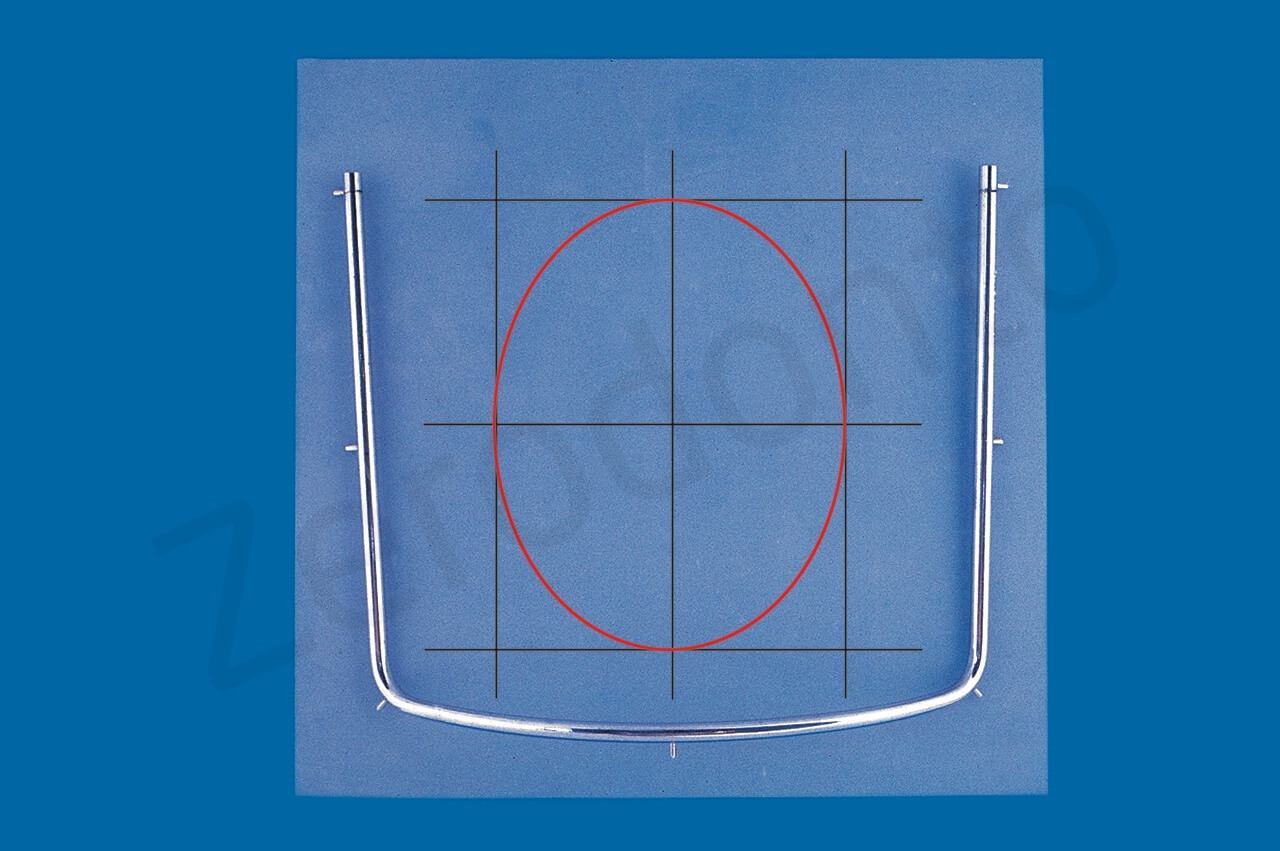
In deciding where to punch the opening in the rubber sheet, one can mentally trace three vertical and three horizontal lines. The ellipse inscribed within the central rectangle corresponds to the two dental arches
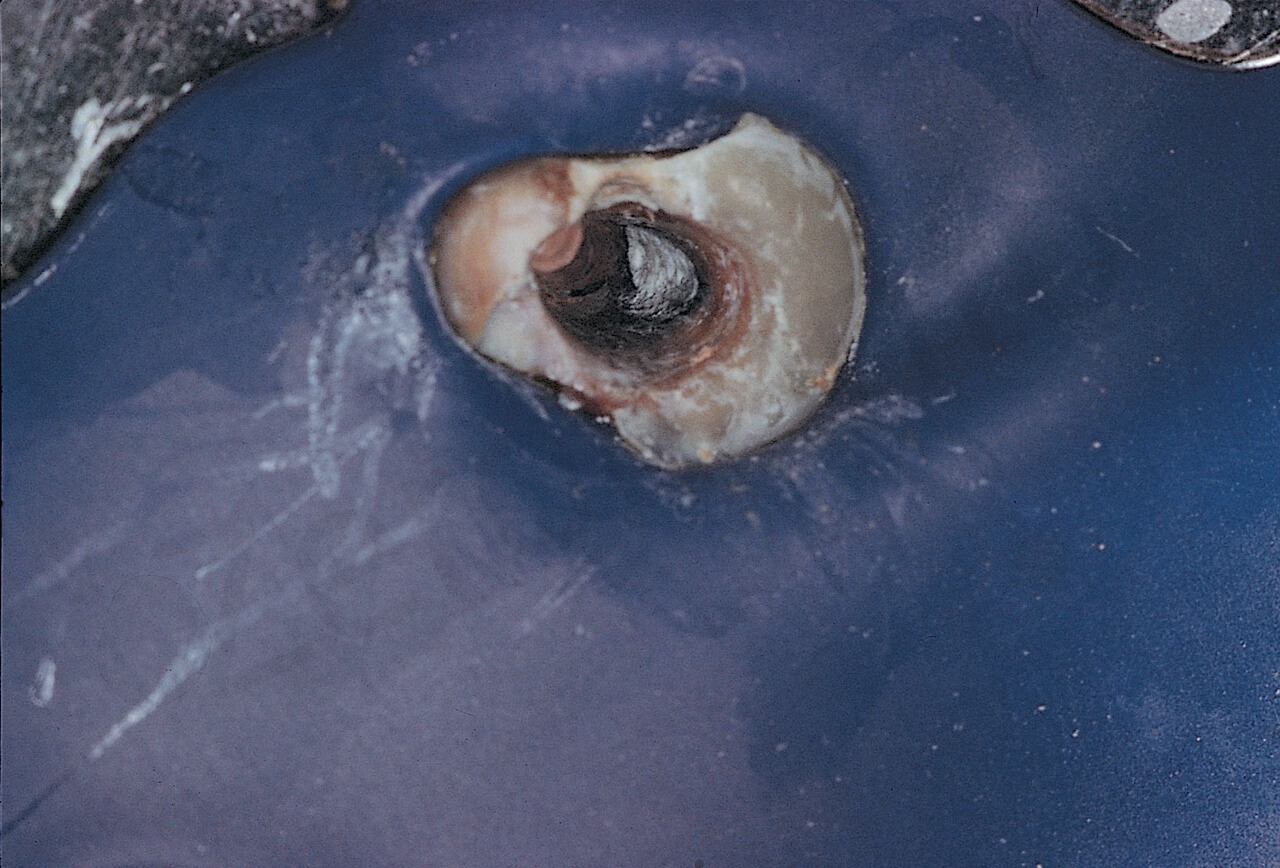
In treating a posterior tooth, it is preferable to place the tooth in the center of the dam, placing the dam asymmetrically with respect to the patient’s face (Fig. 21), rather than the opposite (Fig. 22).

Fig. 21. A. The opening has been made more or less within the center of the dam, which is asymmetrical with respect to the patient’s face

Fig. 21. B. In this way, the metallic frame does not interfere with the X-ray machine

Fig. 21. C. The patient can also breathe through the mouth

Fig. 22. A. The opening has been made at the point indicated by the ellipse rule. The dam is therefore asymmetric with respect to the patient’s face, while the tooth emerges at a point close to the metallic frame

Fig. 22. B. The metallic frame interferes with the X-ray machine, causing it to project the frame’s shadow onto the radiograph

Fig. 22. D. The dam adheres to the entire circumference of the mouth, precluding oral respiration
The more distal the position of the tooth, the closer the opening must be to the center of the rubber sheet.35 It is better that the tooth under treatment be in the center of the operative field than that the rubber be in the center of the mouth.36
Central positioning of the opening has several advantages in treating the molars:
– Once positioned, the dam will be quite asymmetrical with respect to the patient’s mouth, and therefore further displaced from the side being worked on. This insures greater retraction of the lips and ipsilateral cheek.
– Since the dam is asymmetrical, there is enough space from the controlateral part to permit oral respiration on the part of the patient, which is essential in patients who have difficulty with nasal respiration. The dentist can also easily introduce any radiographs into the patient’s mouth that need to be taken intraoperatively without having to dismount the frame of the dam.
– The same space can be useful in the patient with abundant salivation to keep an aspirator in the mouth.
– Because the dam is displaced from the side in which one is working, the risk of obtaining intraoperative radiographs obstructed by the metal frame is reduced.

The metallic frame interferes with the X-ray machine, causing it to project the frame’s shadow onto the radiograph
Before positioning the rubber dam, it is a good idea to illustrate to the patient the utility and function of the dam, especially in very young patients; for example, we can place a fingertip in the dam opening.
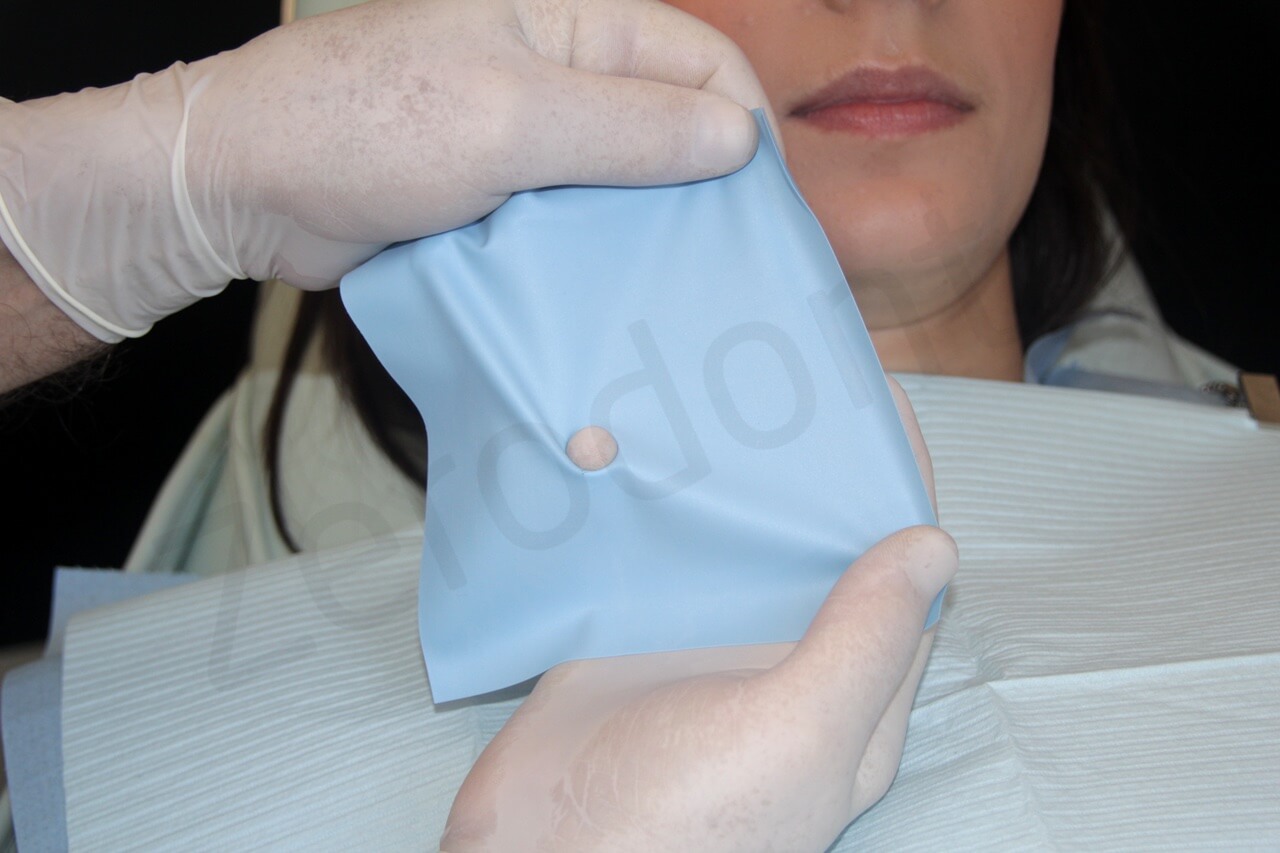
The fingertip is introduced in the dam opening to better illustrate to the patient the functions of this rubber sheet
The patient must also be told that, with the dam in place, he/she may safely swallow, cough, or yawn and that he/she may do so without placing his/her hand in front of the mouth! The only things he/she must not do are talk and rinse his/her mouth.
Patients with an easily-provoked gag reflex should relax since the rubber dam will not touch the areas that may provoke their reflex (base of the tongue and soft palate); still, the dam is definitely better tolerated and safer than cotton rolls.
There are many methods of placing the dam. They are more or less simple, and the dentist can choose the preferred one. The assistant can place the dam around the tooth (Fig. 24) as the dentist positions the clamp (Fig. 25) and then the frame (Fig. 26). This procedure is often difficult, if not impossible, especially in the posterior areas or particularly small mouths.

Fig. 24. The assistant’s hands position the dam directly around the tooth to be treated
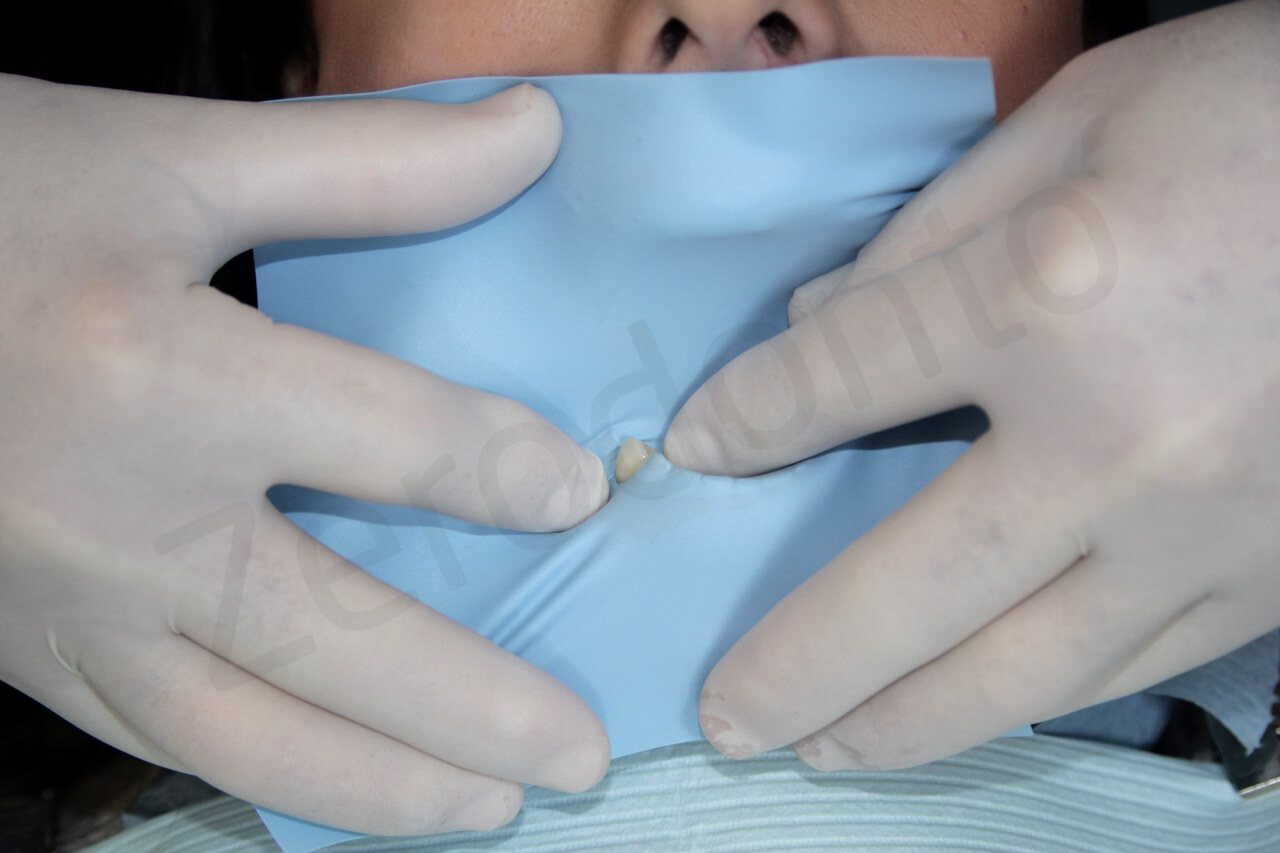
Fig. 24. B. The assistant’s hands position the dam directly around the tooth to be treated

Fig. 25. The dentist positions the clamp

With assistance, the dentist positions Young’s frame
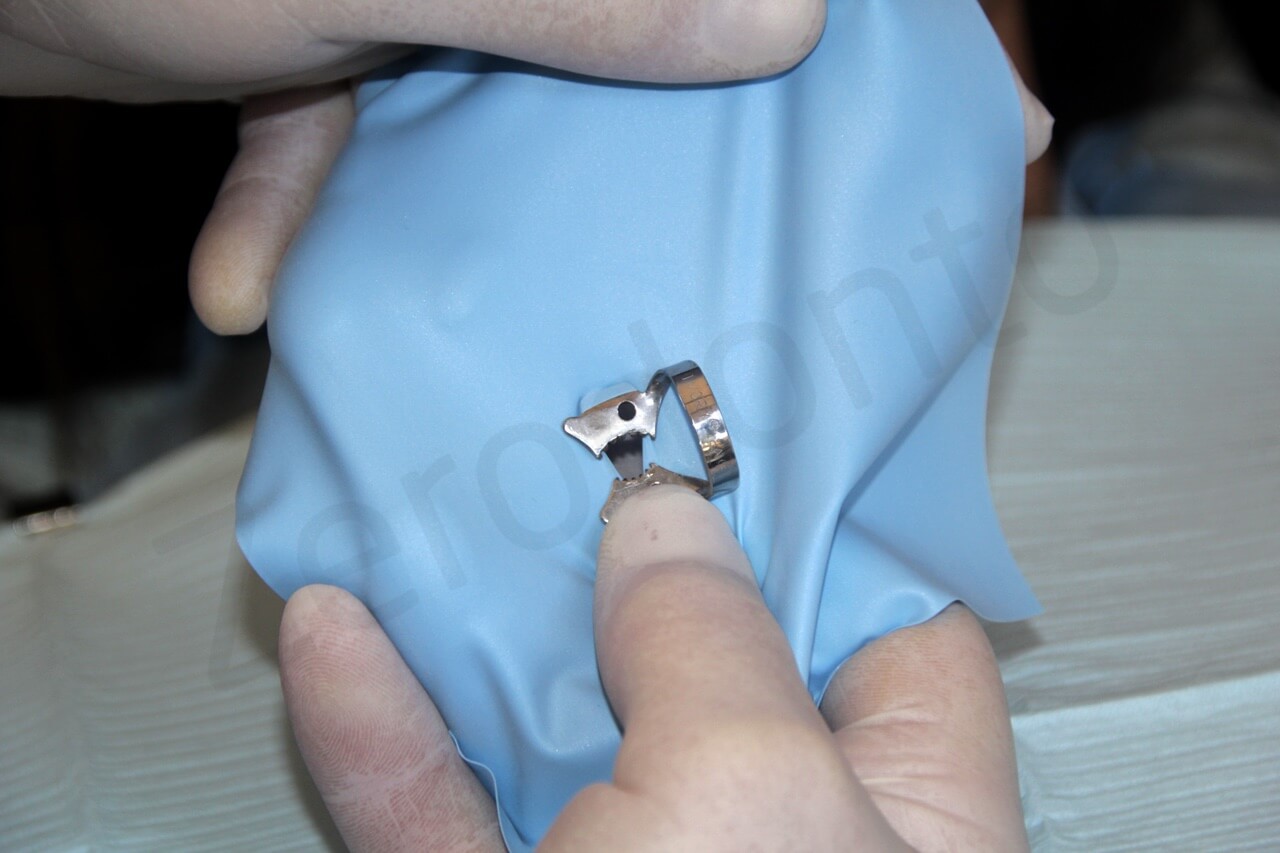
Another method requires placing the clamp within the opening of the dam. Both the clamp and dam are positioned around the tooth, even without an assistant. The positioning of the frame follows. Obviously, in this case the technique varies slightly, depending on whether one uses winged (Fig. 27) or wingless clamps (Fig. 28).

Fig. 27. A. Positioning of the dam can be performed without the help of an assistant. The perforated dam has been stretched over the wings of the clamp

Fig. 27. B. While the dentist’s left hand supports the upper margin of the dam, his right hand positions the clamp around the tooth
Positioning of the rubber dam with an unwinged clamp. The clamp’s arch is passed through the dam’s opening

The rubber dam clamp forceps are introduced into the clamp’s openings

The dam is folded with the clamp at the tip, while the clamp is moved toward the tooth

The clamp has been positioned

The dam is stretched with Young’s frame

The dentist uses his fingers to slide the dam completely below the clamp

The dentist uses his fingers to slide the dam completely below the clamp
One can also put the clamp on a dam that has already been placed onto a frame and position the entire assembly in the patient’s mouth.
Finally, one can place the clamp on the tooth and then slip the framed dam around it. The technique most commonly used is that described in Fig. 11.19.

A wingless clamp has been positioned around the tooth
The rubber sheet has been slid below the clamp, which is already in place

The rubber sheet has been slid below the clamp, which is already in place
Removal of the dam is easy, as all one needs to do is to take away the clamp. If several teeth lie beneath the dam and one of them has a temporary or recent restoration, it is preferable to cut it and extract it from below rather than passing the rubber sheet through this delicate contact area. Once it has been removed, the dam must always be checked so that no small fragments are left below the contact areas.

To facilitate its removal, the dam is cut rather than passed through the interproximal contact
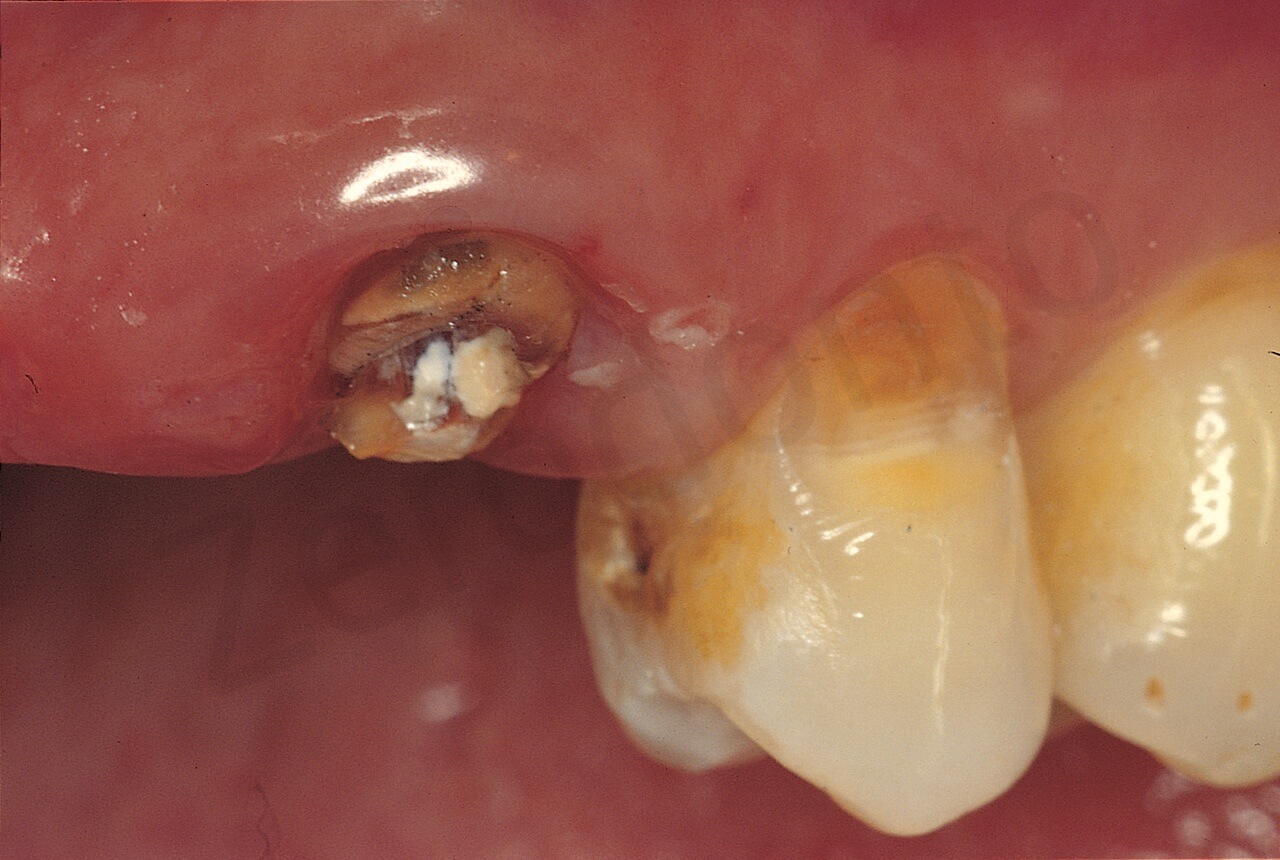
In the case of incompletely erupted teeth that are very conical or where the bulge is apical to the gingival crest, there are no undercuts to prevent the clamp from sliding coronally.
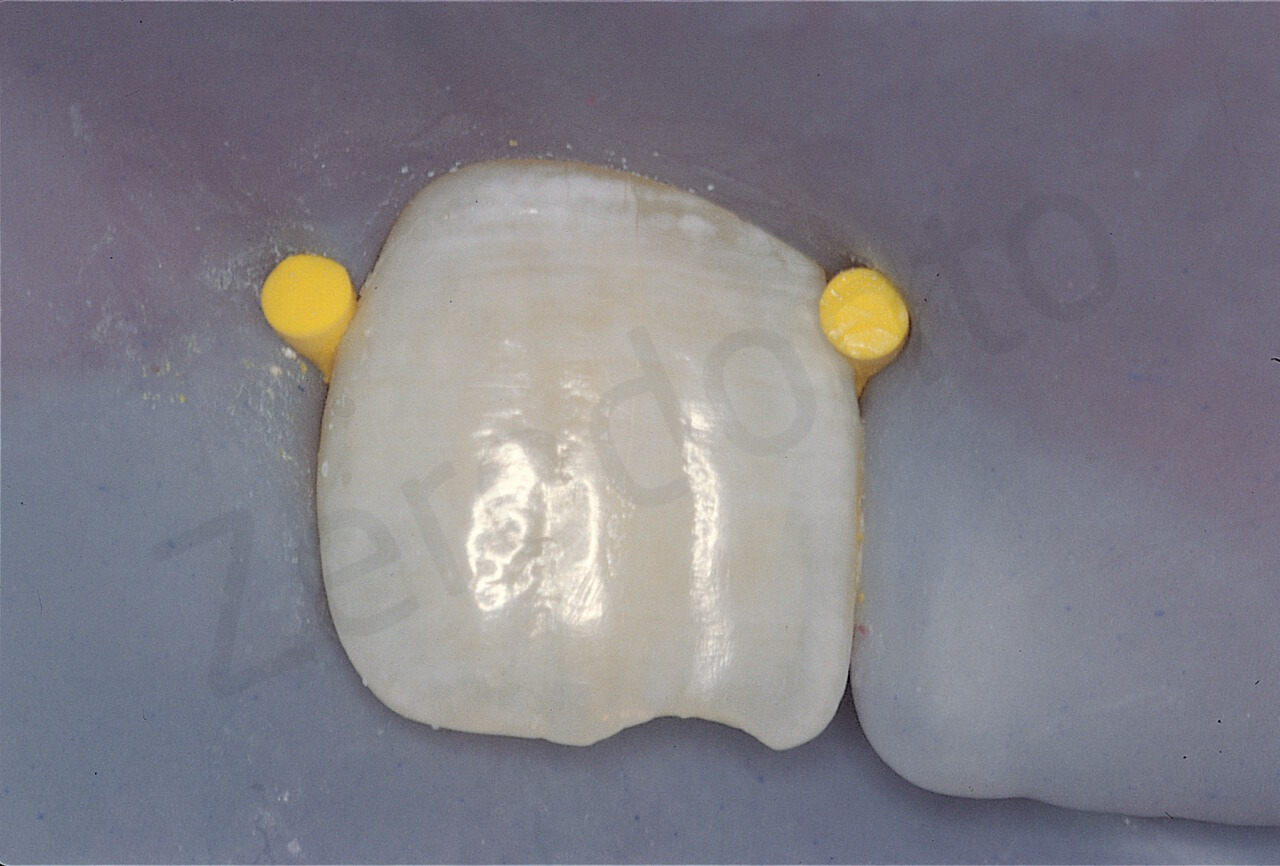
In such cases, one can resort to an expedient that takes a few minutes but allows one to work as one should. One can acid etch the enamel buccally and palatally or lingually to allow the adhesion of two small ribbons of composite resin, which serve as areas which the clamp may grip.37,38
These composite ribbons must not interfere with the periodontium, but must be positioned 1 or 2 mm from the gingival margin to allow positioning of the clamp. The lingual or palatine spots should not interfere with the future access cavity or the occlusion. They will require smoothing, so as not to damage the lips, especially if, as in the case of Fig. 32, they must be left in place for several months and multiple appointment procedures.

Fig. 32. A. The fractured tooth requiring endodontic treatment still has not completely erupted, and its height of contour is still apical to the gingival margin. To position the rubber dam clamp, it was necessary to polymerize two spots of composite resin on the buccal and palatal enamel
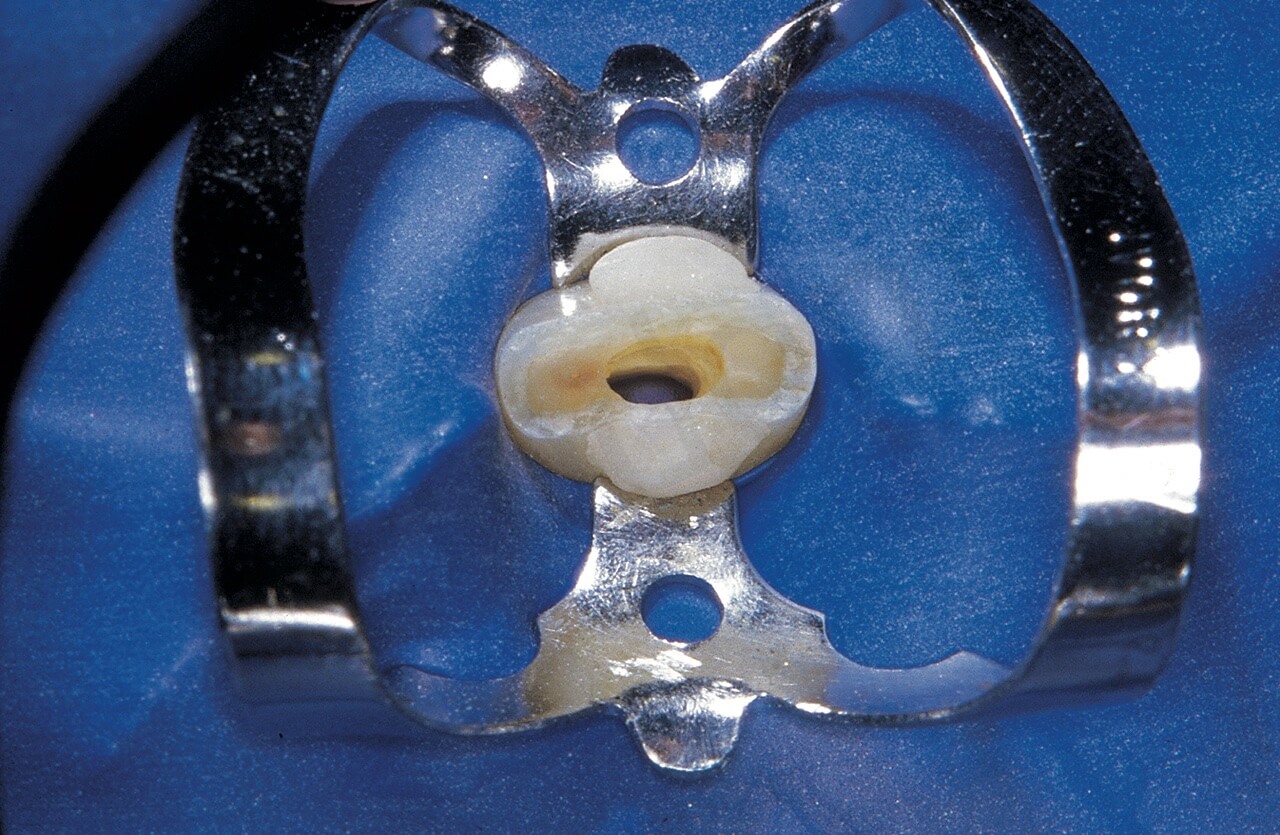
Fig. 32. B. Access cavity created on the fracture rim. Note the two composite spots that hold the clamp in position
In the case of very damaged teeth which require immediate attention, such as for esthetic reasons, it may be useful to anchor the dam to the adjacent teeth.

The dam has been placed on the canine and central incisor to allow endodontic therapy of the root of the lateral incisor
The dam’s stability can also be maintained with the help of small rubber fragments of the rubber dam itself, which are passed below the contact areas of the adjacent teeth.

The dam is kept in place by a clamp positioned on the mesial tooth and by a fragment of the dam which has been passed beneath the distal contact area of the distal tooth
In particularly crowded teeth, such fragments may even substitute for the dam clamps.

Since the front teeth of this patient were so crowded, there was no space for the clamps. The dam is kept in place by two fragments of the dam which have been passed under the distal contact areas of the lateral incisors
Special elastic wires are also available in different thickness, to stabilize the dam in the same way.

Elastic wires of different thickness to keep the rubber dam in place (Hygenic Corporation, Ohio)
The clamp was interfering with the mirror used in this particular case for documentation purposes, therefore the elastic wires were used

The clamp was interfering with the mirror used in this particular case for documentation purposes, therefore the elastic wires were used
When treating endodontically a bridge abutment or a tooth with an intracoronal splinting or orthodontic wire, one can use various techniques to ensure that the dam isolates the field from saliva well:
– Suturing of the dam below the connections of the prosthesis or splinting.39,40
– Use of cavity varnishes (for small defects), cavit, Orabase,35 oral adhesives, periodontal dressing,41 Rubber base adhesive,42 mixture of denture adhesive and zinc oxide powder (PGZ),43 Oraseal (Fig. 37 – 39) or light cured “liquid” rubber dam (Fig. 40). The last mentioned is the material of choice, because it is very easy to use.

Fig. 37. Oralseal (Ultradent)
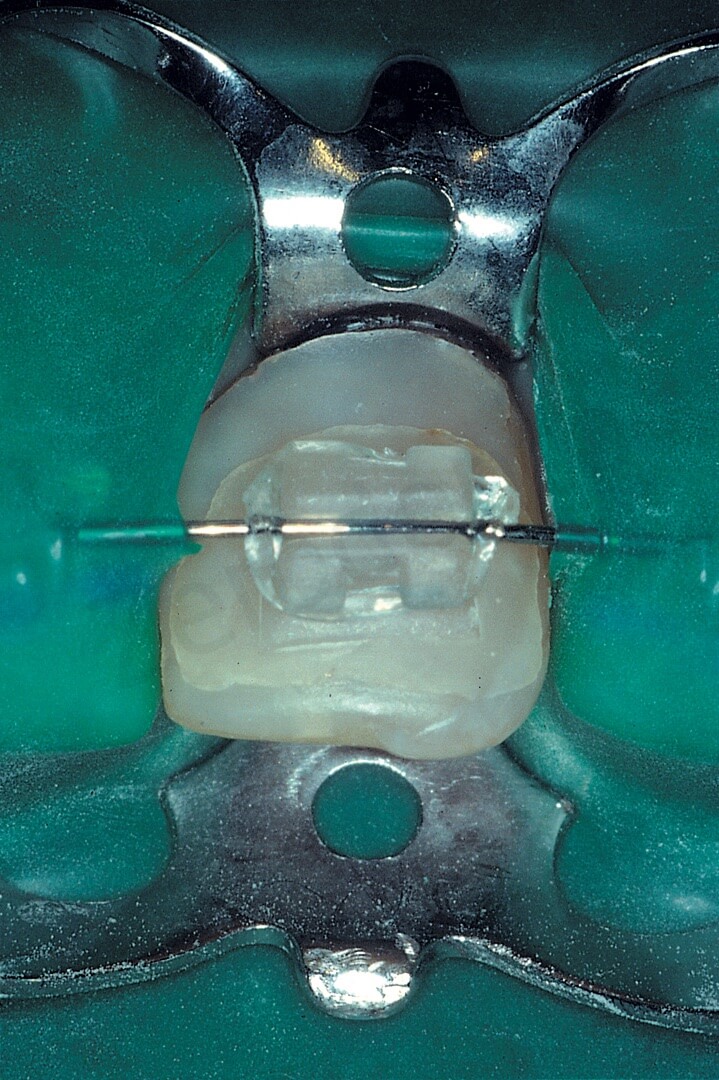
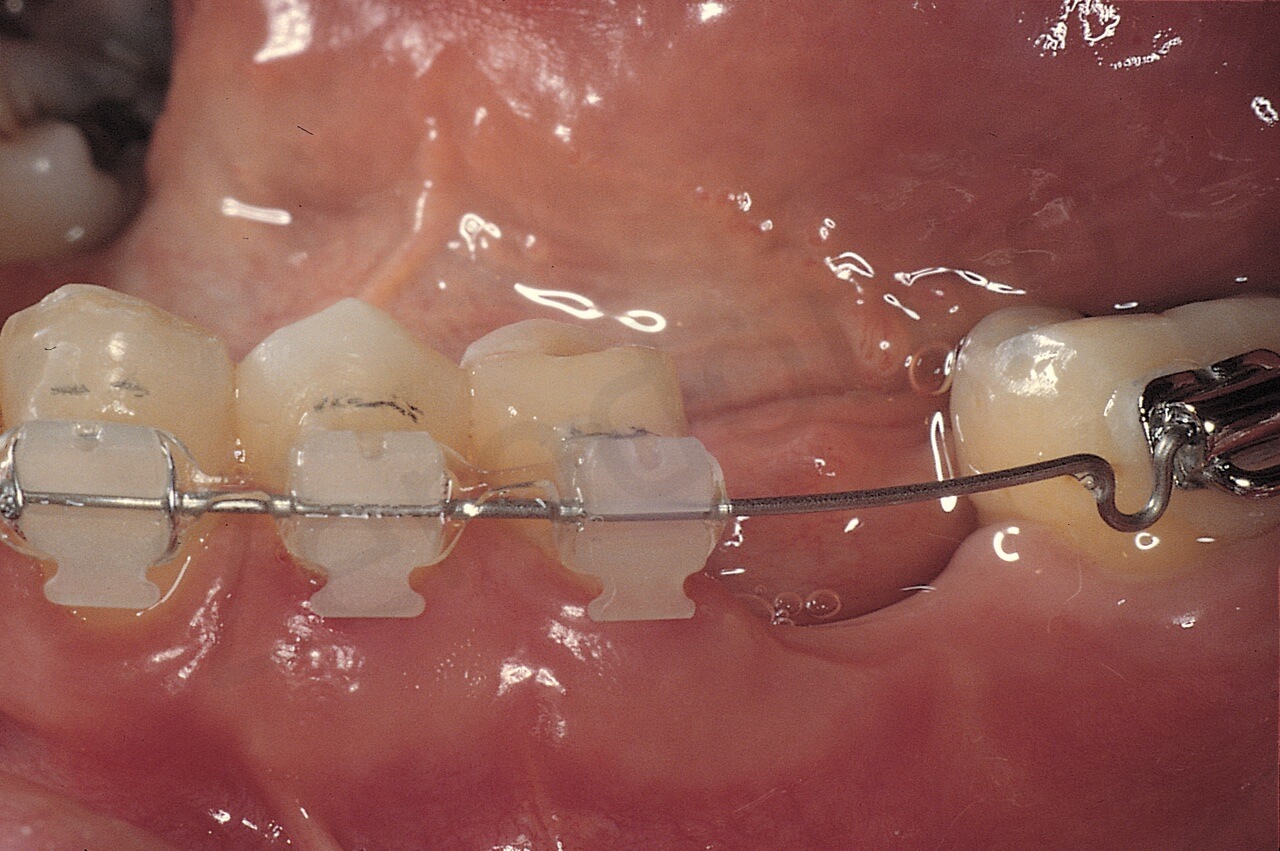
Fig. 38. A. The orthodontic wire precludes tight sealing of the rubber sheet.

Fig. 38. B. A tight seal has been achieved with Oraseal
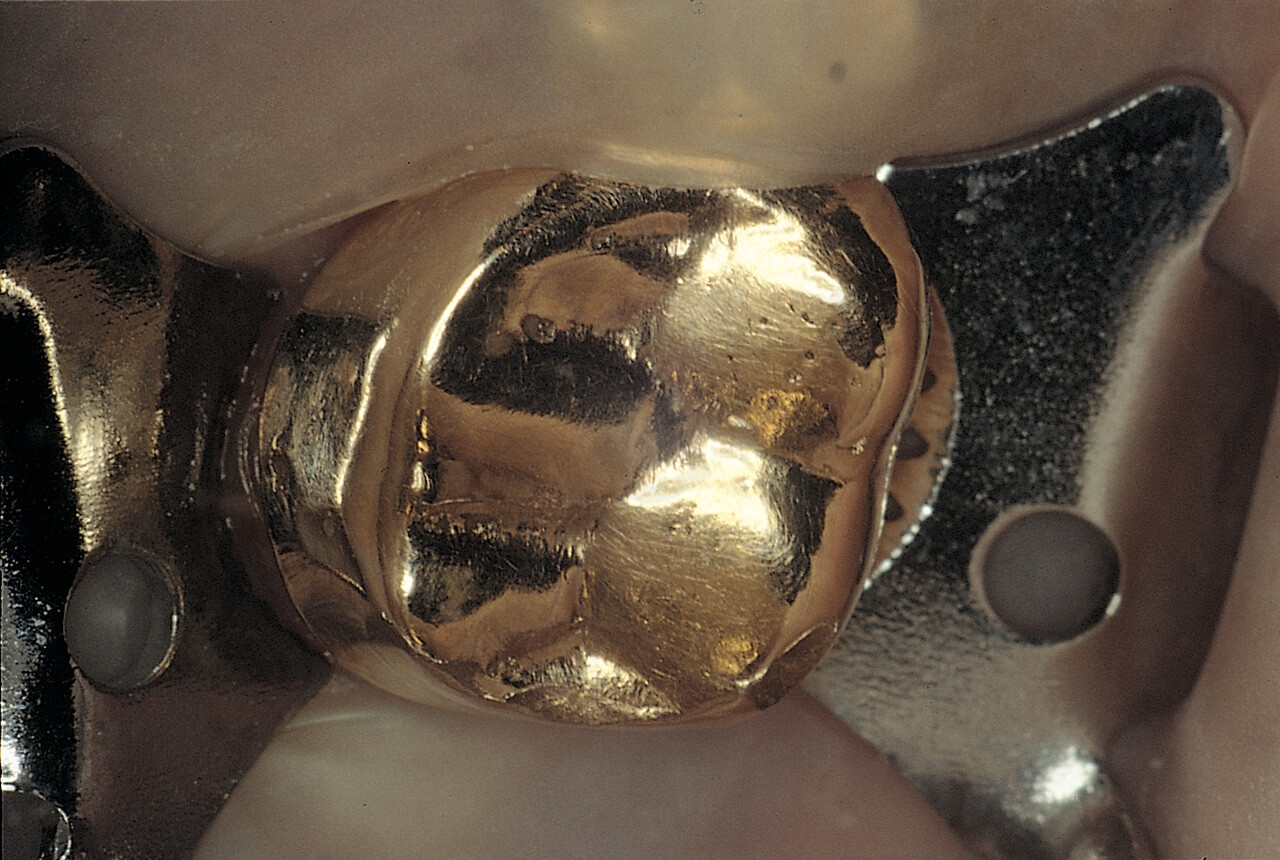
Fig. 39. A. The presence of the welding hampers the dam from passing below the contact area.
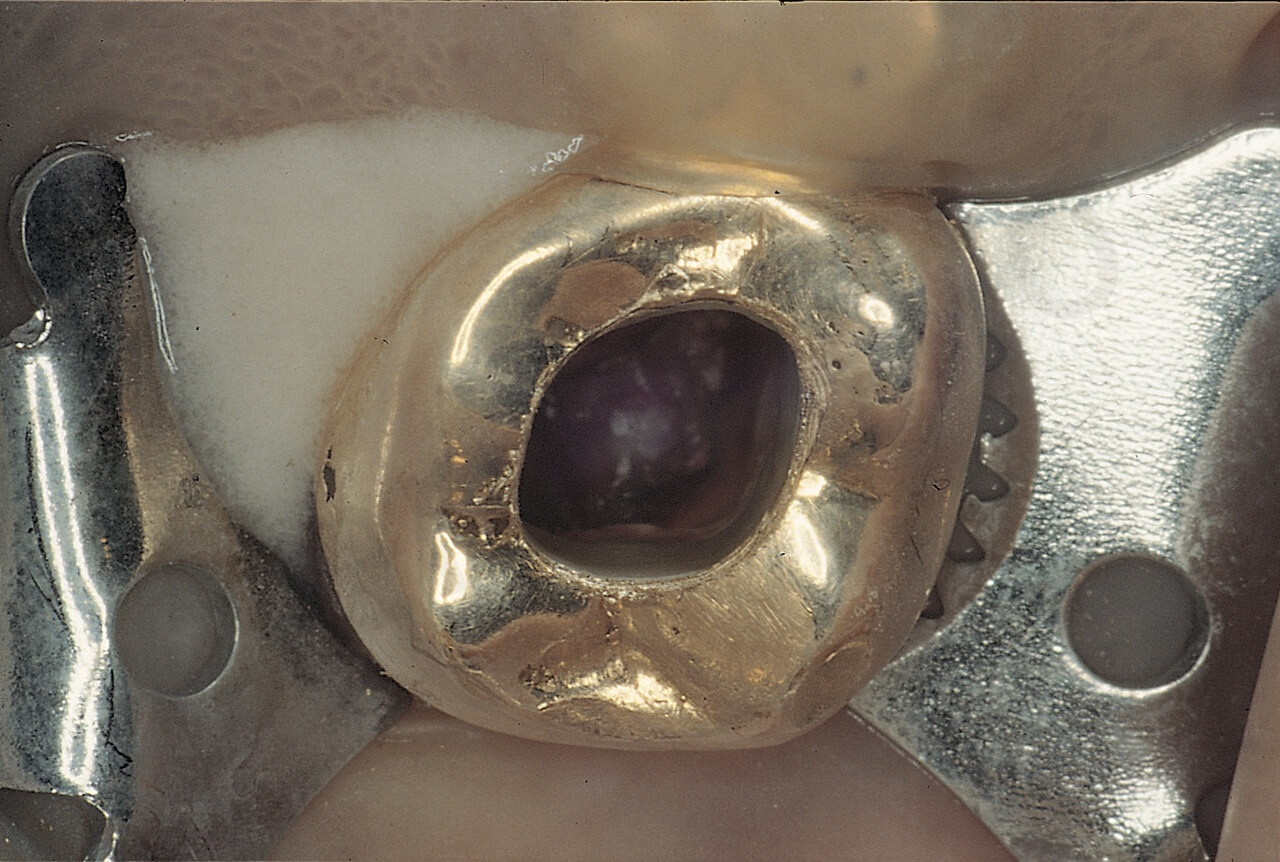
Fig. 39. B. Oraseal helps to obtain an equally good seal.

The light cured “liquid” rubber dam (Opaldam, Ultradent) is the material of choice to improve the sealing of leaking rubber dams
In the case in which the tooth under treatment is connected to the adjacent teeth by orthodontic wire, one can try to position the clamp above the orthodontic attachment and wire.
The lower left second premolar requires endodontic therapy. Occlusal view
Buccal view

Positioning the clamp below the orthodontic attachment, the dam straddles the wire and therefore does not seal
Positioning the clamp below the orthodontic attachment, the dam straddles the wire and therefore does not seal

The clamp has been positioned above the orthodontic attachment and wire; thus, the dam seals perfectly

The clamp has been positioned above the orthodontic attachment and wire; thus, the dam seals perfectly
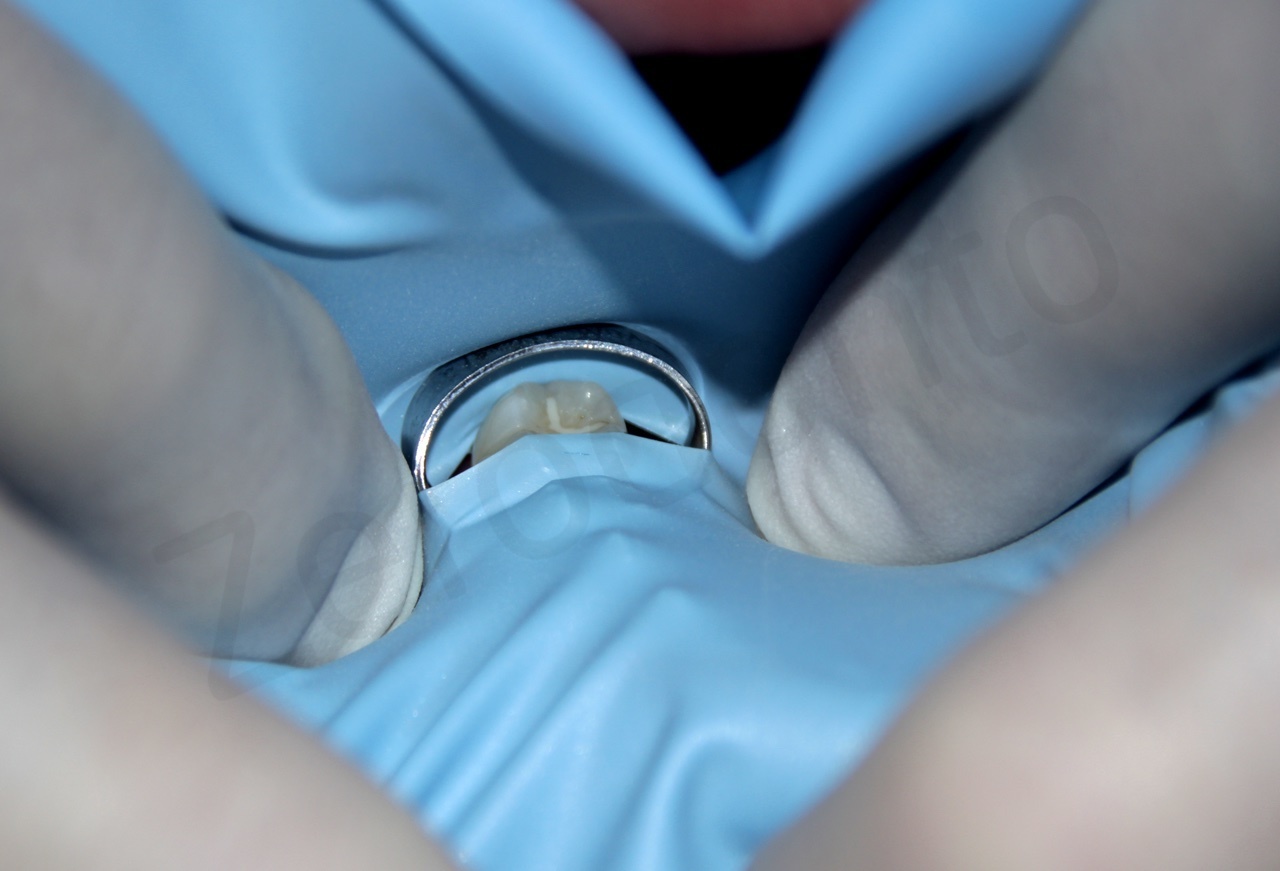
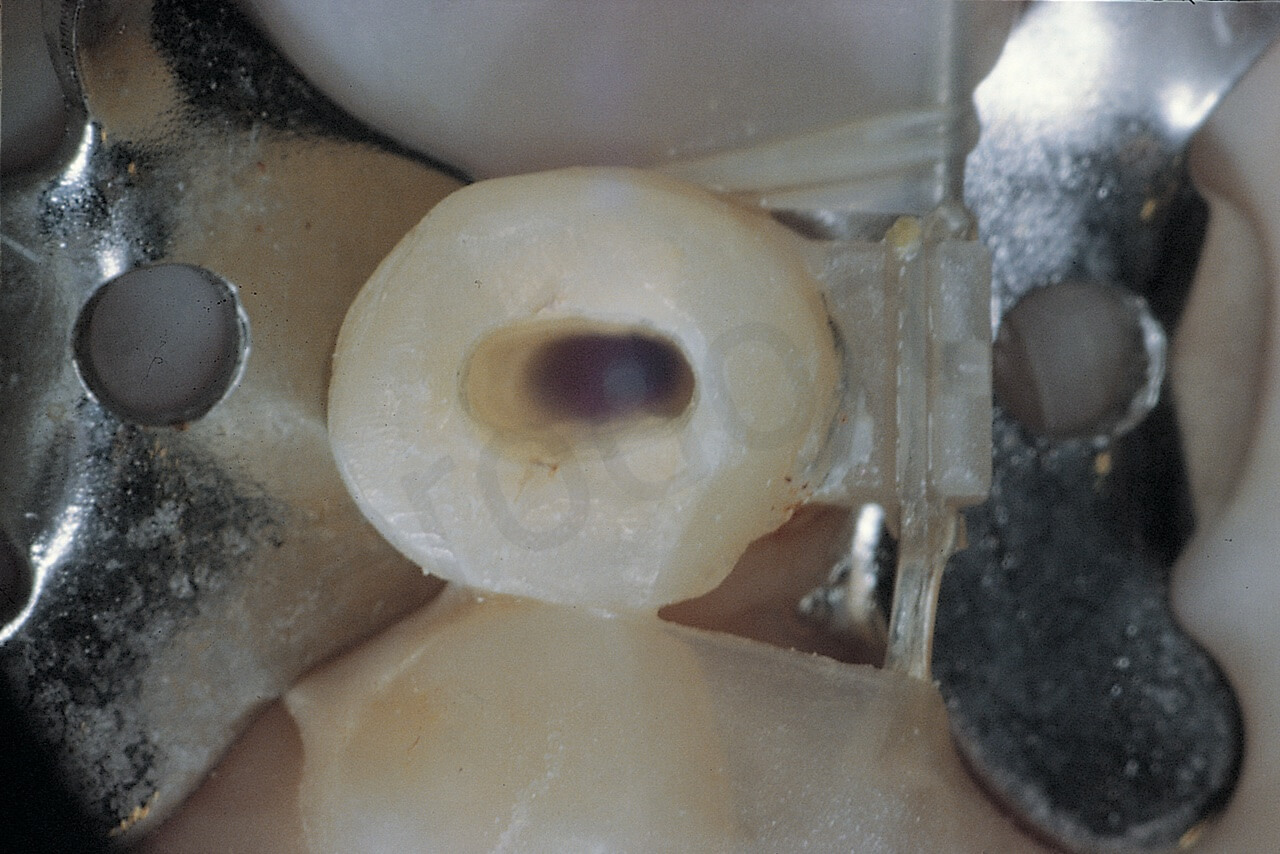
If the tooth requiring endodontic treatment is particularly damaged, so that the clamp cannot be positioned stably, it must be pre-treated so as to allow adequate positioning of the rubber dam. An easy and fast way to pre-treat the damaged tooth is curing a “collar” of composite which, through dentin bonding, will be polimerized on the dentin after acid etching with ortophosphoric acid.
The upper left cuspid has no crown. The patient had esthetic problems, which precluded a crown lenghtening procedure to be done before the endodontic retreatment

The clamp has been positioned on the adjacent premolar and also the two central incisors have been isolated. A small “collar” of composite has been cured on the buccal aspect of the root of the cuspid
The clamp has been positioned on the adjacent premolar and also the two central incisors have been isolated. A small “collar” of composite has been cured on the buccal aspect of the root of the cuspid

The same kind of pretreatment was done to the first molar, to have a more stable rubber dam clamp

The same kind of pretreatment was done to the first molar, to have a more stable rubber dam clamp
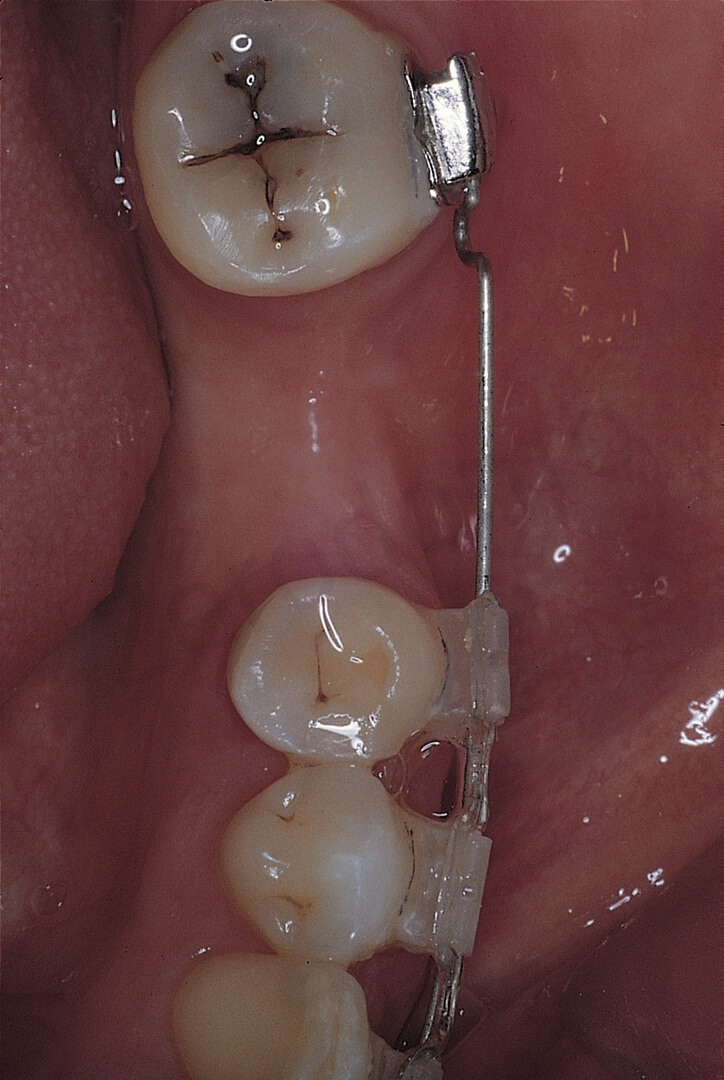
Another suggestion could be positioning the clamp on a distal tooth, so that the elasticity of the dam doesn’t interfere with the tooth to be treated, where a second clamp can be gently positioned.

The upper right second premolar has a 45° crown fracture and the 90N clamp keeps sliding under the tension of the rubber sheet. One clamp has been positioned on the second molar and another one (90N) on the second premolar to be treated. Now the elasticity of the dam is pulling on the molar and not at all on the premolar
Bibliography
- HARRIS, C.H.: Principles and practice of Dentistry. 11th P. Blakiston, Son & Co.. Philadelphia, 1885.
- ANDRIEU, E.: Traité de Dentisterie Operatorie. Octave Doin, Editeur, Paris, 1889
- AMERICAN ASSOCIATION OF ENDODONTISTS: AAE Position Statement, 2010.
- EUROPEAN SOCIETY OF ENDODONTOLOGY: Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int. Endod. J. 39:921-30, 2006.
- HELING, B., HELING, I.: Endodontic procedures must never be performed without the rubber dam. Oral Surg. 43:464, 1977.
- CAMERON, S.M., WHITLOCK, W.L., TABOR, M.S.: Foreign body aspiration in dentistry: a review. J. Am. Dent. Assoc. 127:1224, 1996.
- ISRAEL, H.A., LEBAN, S.G.: Aspiration of an endodontic instrument. J. Endod. 10:452, 1984.
- LAMBRIANIDIS, T., BELTES, P.: Accidental swallowing of endodontic instruments. Endo. Dent. Traumatol. 12:301, 1996
- MEJIA, J.L., DONADO, J.E., POSADA, A.: Accidental swallowing of a dental clamp. J. Endod. 22:619, 1996.
- TAINTOR, J.F., BIESTERFELD, R.C.: A swallowed endodontic file: case report. J. Endod. 4:254, 1978.
- SUSINI, G., POMMEL, L., CAMPS, J.: Accidental ingestion and aspiration of root canal instruments and other dental foreign bodies in a French population. Int Endod J; 40(8):585-9, 2007.
- HILL, E.E., RUBEL, B.: A practical review of prevention and management of ingested/aspirated dental items. Gen Dent 56(7):691-4, 2008.
- FREDEKIND, R.E., McCONNEL, T.A., JACOBSEN, P.L.: Ingested objects: a case report with review of management and prevention. Calif Dent Assoc 23(9):50-55, 1995.
- KUO, S.C., CHEN, Y.L.: Accidental swallowing of an endodontic file. Int Endod J; 41(7):617-22, 2008.
- GOULTSCHIN, J., HELING, B.: Accidental swallowing of an endodontic instrument. Oral Sur Oral Med Oral Path 32(4): 621-2, 1971.
- FORREST, W.R., PEREZ, R.S.: The rubber dam as a surgical drape: protection against AIDS and hepatitis. Gen Dent, 37(3):236-7, 1989.
- COCHRAN, M.A., MILLER, C.H., SHELDRAKE, M.A.: The efficacy of the rubber dam as a barrier to the spread of microorganisms during dental treatment. J Am Dent Assoc, 119(1):141-4, 1989
- KITAMURA, A., NAGAHATH, E. et al.: A misingested hand reamer. Report of case (Abstract). J. Am. Dent. Assoc. 89:169, 1974.
- FOX, J., MOODNIK, R.M.: The case of the missing file. Or six reasonswhy root canal therapymust never be performed without the rubber dam (Abstract). NY State Dent. 32:25, 1966.
- CHRISTEN, A.G.: Accidental swallowing of an endodontic instrument. Oral Surg. 24:684-6, 1967.
- GOULSCHIM, J.P., HELING, B.: Accidental swallowing of an endodontic instrument. Oral Surg. 32:621-2, 1971.
- GOVILA, C.P.: Accidental swallowing of an endodontic instrument. Oral Surg. 48:269-71, 1979.
- BARKEIMER, W.W., COOLEY, R.R., ABRAMS, H.: Prevention of swalloving or aspiration of foreign objects. J. Am. Dent. Assoc. 97:473-6, 1978.
- WAHL, P.: Isolamento del campo e radiologia. L’Informatore Endodontico. 1(1):19, 1997.
- AIELLO, G.: Come mettere la diga sui denti difficili. Il Dentista Moderno 6:1085, 1986.
- BEAUDRY, R.J.: Prevention of rubber dam hypersensitivity. J. Endod. 10:544, 1984.
- DIAS DE ANDRADE, E., RANALI, J., VOLPATO, M.C., MOTTA MAIA DE OLIVEIRA, M.: Allergic reaction after rubber dam placement. J. Endod. 26:182, 2000.
- PATTERSON, C.J.W.: Polydam-polythene sheet, a practical alternative to rubber dam for patients allergic to rubber compounds. Int. Endod. J. 22:252, 1981.
- KNOWLES, K.I., IBARROLA, J., LUDLOW, M.O., ANDERSON, J.R., NEWCOMB, B.E.: Rubber latex allergy and the endodontic patient. .Endod. 24:760, 1998.
- CRAGG, T.K.: The use of rubber dam in endodontics. J. Can. Dent. Assoc., 38:376, 1972.
- LAVAGNOLI, G.: La cavità d’accesso. Dental Cadmos, 1:17, 1984.
- REUTER, J.F.: The isolation of teeth and the protection of the patient during endodontic treatment. Int. Endod. J., 16:173, 1983.
- GALLO, G.G.: La diga. VII Congresso Internazionale della Società Italiana di Endodonzia. Tavola clinica. Chiavari. Novembre 1986.
- PECCHIONI A.: Endodonzia. Manuale di tecnica operativa. IV ed. I.C.A., 1986, p. 36.
- SCHWARTZ, S.F.: Preparation for therapy. In: Cohen S. and Burns R.C. eds. Pathways of the pulp. 3rd ed. St. Louis, The C.V. Mosby Company, 1984, p. 93.
- BENCE, R.: Handbook of clinical endodontics. 2nd ed. St. Louis, The C.V. Mosby Company, 1980. pag. 80.
- GREENE, R.R., SIKORA, F.A., HOUSE, J.R.: Rubber dam application to crownless and cone-shaped teeth. J. Endod., 10:82, 1984.
- WAKABAYASHI, H., OCHI, K., TACHIBANA, H., MATSUMOTO, K.: A clinical technique for retention of a rubber dam clamp. J. Endod. 12:422, 1986.
- ANTRIM, D.D.: Rubber dam isolation of fixed prostheses. J. Endod., 8:521, 1982.
- LIEDENBERG, W.H.: Manipulation of rubber dam septa: an aid to the meticulous isolation of splinted prostheses. J. Endod. 21:208, 1995.
- WEINE, F.S.: Endodontic therapy. 3rd ed. St. Louis, The C.V. Mosby Company, 1982, p. 255.
- BRAMWELL, J.D., HICS, M.L.: Solving isolation problems with rubber base adhesive. J. Endod., 12:363, 1986.
- WEISMAN, M.I.: Remedy for dental dam leakage problems. J. Endod. 17:88, 1991.
- FRESA, R.: Il consenso informato in Odontoiatria. G. Ediz. Medico Scientifiche, Torino. 1998, p.230.
